Nursing care plans are the cornerstone of effective patient care, providing a structured, systematic approach to identify patient needs, formulate diagnoses, and implement targeted interventions. For nursing professionals and students alike, mastering the art of crafting robust nursing care plans is essential for delivering high-quality, patient-centered care. This guide will walk you through the intricacies of developing comprehensive nursing care plans, with a specific focus on nursing diagnoses and interventions.
What is a Nursing Care Plan?
A nursing care plan (NCP) is a formal, dynamic document that outlines a patient’s healthcare needs, the nursing diagnoses that address these needs, the desired patient outcomes, and the specific nursing interventions required to achieve those outcomes. It serves as a vital communication tool amongst the healthcare team, ensuring consistency and coordination of care. At its core, the nursing care plan facilitates a systematic approach to diagnosis and intervention, ensuring that patient care is not only reactive but also proactive and preventative. Without a well-defined care plan, the quality and consistency of patient care can be significantly compromised, leading to fragmented and potentially less effective treatment.
The process of nursing care planning is not a one-time event. It begins upon a patient’s admission and is continuously revised and updated in response to the patient’s evolving condition and the evaluation of progress towards established goals. This ongoing adaptation ensures that the care plan remains relevant and effective throughout the patient’s healthcare journey. The ability to plan and deliver individualized, patient-centered care is the hallmark of excellent nursing practice, and the nursing care plan is the primary tool to achieve this.
Types of Nursing Care Plans
Nursing care plans can be broadly categorized into informal and formal plans, and further subdivided into standardized and individualized formal plans.
- Informal Nursing Care Plans: These are mental strategies or action plans that nurses develop in their minds as they think about a patient’s needs and care. They are not written down and are often based on the nurse’s immediate assessment and experience.
- Formal Nursing Care Plans: These are written or computerized guides that systematically organize patient information, nursing diagnoses, goals, and interventions. Formal care plans ensure clear communication and consistent care delivery.
Formal care plans are further classified into:
- Standardized Care Plans: These are pre-written care plans that outline the nursing care for patients with common needs or medical conditions. They provide a general framework for care and are designed to ensure consistent practice for frequently encountered patient populations. Standardized plans are efficient for addressing routine needs but may not fully address the unique complexities of individual patients.
- Individualized Care Plans: These plans are tailored to meet the specific and unique needs of an individual patient. They are developed by adapting standardized care plans or creating entirely new plans based on a comprehensive assessment of the patient’s specific health status, preferences, and goals. Individualized care plans are crucial for providing holistic and patient-centered care, especially for patients with complex or unusual needs.
Standardized Care Plans
Standardized care plans are valuable resources developed by healthcare agencies to ensure a baseline level of quality and consistency in patient care. They are particularly useful for patients with common medical diagnoses or needs, as they provide a pre-approved set of nursing diagnoses, desired outcomes, and interventions. By utilizing standardized plans, nurses can efficiently address routine aspects of care, freeing up time to focus on more complex and individualized patient needs. These plans serve as a starting point and ensure that essential care elements are not overlooked.
However, it’s crucial to recognize that standardized care plans are not designed to be a one-size-fits-all solution. They lack the specificity to address the nuances of each patient’s unique situation. Therefore, standardized care plans often serve as a foundation upon which nurses build individualized care plans, tailoring them to the patient’s specific circumstances. The care plans listed later in this guide are examples of standardized care plans that can be adapted and individualized.
Individualized Care Plans
An individualized care plan represents the pinnacle of patient-centered care. It involves a meticulous process of adapting a standardized care plan or creating a completely original plan to precisely match the unique needs, preferences, and goals of an individual patient. This process starts with a thorough assessment to identify the patient’s specific health challenges, strengths, resources, and values. The nursing diagnoses, desired outcomes, and interventions are then carefully selected and customized to address these specific factors.
Individualized care plans are essential for providing holistic care, acknowledging the patient as a whole person with physical, psychological, social, and spiritual dimensions. This approach not only optimizes the effectiveness of care but also significantly enhances patient satisfaction. When patients perceive that their care is specifically designed for them, they feel more valued and involved in their healthcare journey. This sense of personalized attention and responsiveness is increasingly important in today’s healthcare landscape, where patient satisfaction is a key indicator of quality care.
Tips for Individualizing Nursing Care Plans:
- Incorporate Patient Preferences: Actively solicit and integrate the patient’s values, beliefs, and preferences regarding their care.
- Address Unique Needs: Identify and address needs that are not covered by standardized plans, such as cultural considerations, lifestyle factors, or specific emotional or psychological concerns.
- Collaborate with the Patient and Family: Involve the patient and their family in the planning process to ensure the plan aligns with their goals and understanding.
- Regularly Review and Revise: Continuously evaluate the plan’s effectiveness and adjust it based on the patient’s changing condition and feedback.
Objectives of Nursing Care Plans
The objectives of writing a nursing care plan are multifaceted and contribute significantly to the quality and effectiveness of patient care:
- Promote Evidence-Based Care: Care plans encourage the use of current best practices and research findings in nursing care, ensuring patients receive the most effective interventions. This evidence-based approach helps standardize high-quality care across different settings.
- Support Holistic Care: Nursing care plans facilitate a holistic approach by considering the patient’s physical, psychological, social, and spiritual needs. This comprehensive perspective ensures that care addresses the whole person, not just the disease.
- Establish Care Pathways and Bundles: Care plans can be used to develop structured care pathways and care bundles for specific conditions. Care pathways streamline care delivery through team consensus on standards and expected outcomes. Care bundles focus on implementing best practices for specific diseases to improve outcomes.
- Clearly Define Goals and Expected Outcomes: Care plans require the articulation of specific, measurable goals and expected outcomes. This clarity provides direction for interventions and allows for objective evaluation of patient progress.
- Enhance Communication and Documentation: Care plans serve as a central communication tool for the healthcare team, ensuring everyone is informed about the patient’s needs and the plan of care. They also provide a framework for documenting the care provided and the patient’s responses.
- Measure Nursing Care Effectiveness: By outlining expected outcomes and documenting progress, care plans provide a mechanism to evaluate the effectiveness of nursing interventions and make necessary adjustments to improve patient outcomes.
Purposes of a Nursing Care Plan
Nursing care plans serve several critical purposes that underscore their importance in modern healthcare:
- Defines the Nurse’s Role: Care plans clearly delineate the unique and independent role of nurses in patient care. They highlight the nurse’s responsibility in addressing patients’ overall health and well-being, beyond simply following physician’s orders.
- Provides Direction for Individualized Care: A care plan acts as a roadmap for delivering personalized care. It guides nurses in critically thinking about and developing interventions that are directly tailored to each patient’s specific needs and circumstances.
- Ensures Continuity of Care: By documenting the patient’s needs and planned interventions, care plans enable nurses across different shifts and departments to provide consistent, high-quality care. This continuity is crucial for maximizing the benefits of treatment and preventing gaps in care.
- Coordinates Care: Care plans facilitate collaboration among all members of the healthcare team. They ensure that everyone is aware of the patient’s care needs and the actions required to meet them, promoting a unified and cohesive approach to care.
- Legal Documentation: Care plans serve as legal documentation of the nursing care provided. They accurately outline assessments, nursing actions, and patient education. Proper documentation in the care plan is essential to demonstrate that appropriate care was delivered.
- Guides Staff Assignment: Care plans can inform staffing decisions by highlighting patients with complex needs that require nurses with specific skills or expertise. This ensures that patients receive care from the most qualified personnel.
- Monitors Patient Progress: Care plans provide a framework for tracking a patient’s progress towards their goals. Regular evaluation allows for timely adjustments to the care plan in response to changes in the patient’s health status or goals.
- Supports Reimbursement: Insurance companies often use medical records, including care plans, to determine reimbursement for healthcare services. Well-documented care plans can justify the medical necessity and appropriateness of the care provided.
- Defines Patient Goals: Care plans promote patient involvement in their care by explicitly stating patient goals. This collaborative approach empowers patients and enhances their adherence to the care plan, leading to better outcomes.
Components of a Nursing Care Plan
A comprehensive nursing care plan typically includes several key components, each playing a vital role in guiding patient care:
- Nursing Diagnoses: These are clinical judgments about individual, family, or community experiences/responses to actual or potential health problems/life processes. Nursing diagnoses provide the basis for selecting nursing interventions to achieve outcomes for which nurses are accountable. They are derived from patient assessment data and are standardized using taxonomies like NANDA-I.
- Desired Outcomes: These are specific, measurable, achievable, relevant, and time-bound (SMART) statements that describe the expected changes in the patient’s health status as a result of nursing care. Outcomes are patient-centered and provide criteria for evaluating the effectiveness of interventions.
- Nursing Interventions: These are the actions that nurses will perform to achieve the desired patient outcomes. Interventions should be evidence-based, safe, and individualized to the patient’s needs and preferences. They can be independent, dependent, or collaborative.
- Rationales: For student care plans, rationales or scientific explanations are included to justify the selected nursing interventions. They link the interventions to underlying pathophysiological or psychological principles, enhancing the student’s understanding of the care plan.
- Evaluation: This component involves assessing the patient’s progress towards achieving the desired outcomes. Evaluation is an ongoing process that determines the effectiveness of the care plan and informs decisions about whether to continue, modify, or discontinue interventions.
Care Plan Formats
Nursing care plans can be organized in various formats, with the most common being three-column, four-column, and student care plan formats. The chosen format often depends on agency preferences or educational requirements.
Three-Column Format
The three-column format is a simplified approach that efficiently organizes key care plan elements. It typically includes columns for:
- Nursing Diagnosis: This column lists the identified nursing diagnoses for the patient.
- Outcomes and Evaluation: This column combines desired patient outcomes and the evaluation criteria for assessing progress towards those outcomes.
- Interventions: This column outlines the specific nursing interventions planned to address each nursing diagnosis and achieve the desired outcomes.
Three-column nursing care plan format
Four-Column Format
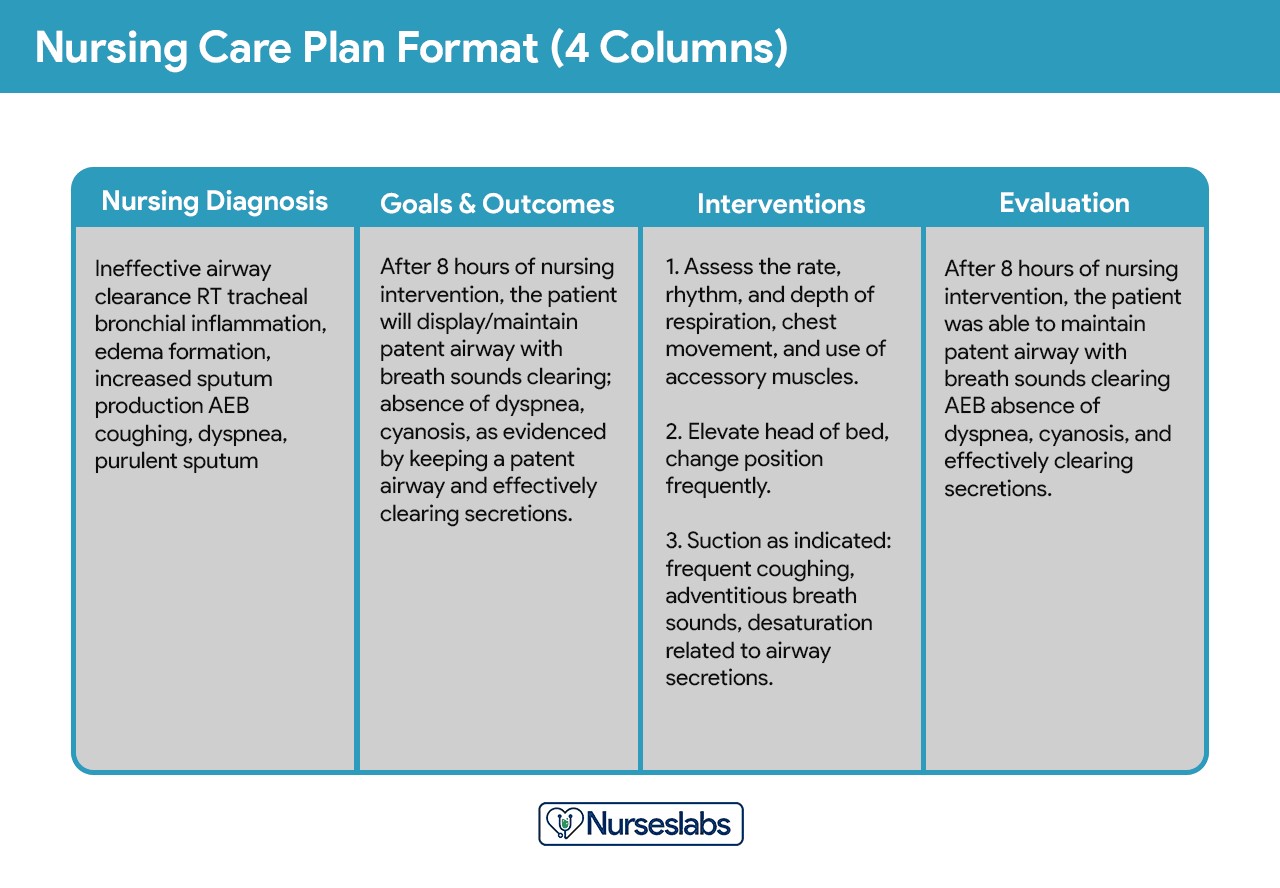
The four-column format provides a more detailed structure, separating outcomes and evaluation into distinct columns. This format is widely used and includes columns for:
- Nursing Diagnosis: Similar to the three-column format, this column lists the nursing diagnoses.
- Goals and Outcomes: This column specifies the desired patient goals and the expected outcomes that indicate goal achievement.
- Interventions: This column details the nursing interventions designed to achieve the stated goals and outcomes.
- Evaluation: This column is dedicated to documenting the evaluation of patient progress towards the outcomes and the effectiveness of the interventions.
Four-column nursing care plan template
You can download sample templates for different nursing care plan formats here:
Download: Printable Nursing Care Plan Templates and Formats
Student Care Plans
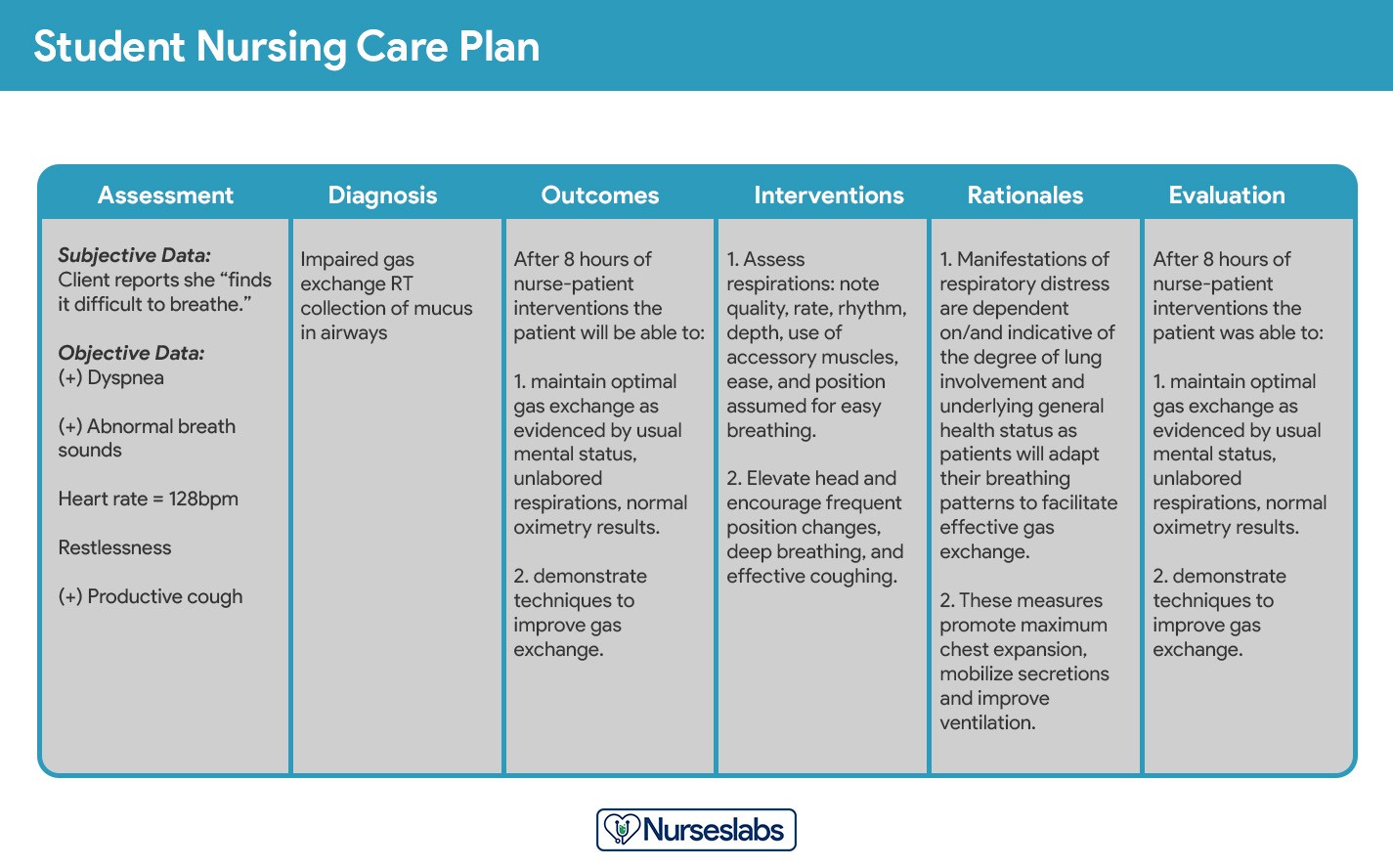
Student care plans are designed for educational purposes and are typically more detailed and comprehensive than those used by practicing nurses. They serve as a learning tool to help students develop critical thinking and care planning skills.
Student nursing care plans are more detailed.
Key features of student care plans include:
- Handwritten Requirement: Often required to be handwritten to reinforce the learning process and promote thoroughness.
- Rationale Column: Includes an additional column for “Rationale” or “Scientific Explanation” after the interventions column. This column requires students to explain the scientific basis for each chosen intervention, strengthening their understanding of the underlying principles of care.
- Detailed Assessment Data: Student care plans typically require more extensive documentation of assessment data to demonstrate a comprehensive understanding of the patient’s condition.
Writing a Nursing Care Plan: Step-by-Step Guide
Creating an effective nursing care plan involves a systematic, step-by-step approach. Each step builds upon the previous one, ensuring a logical and patient-centered plan. Here’s a detailed guide to writing a nursing care plan:
Step 1: Data Collection or Assessment
The foundational step in developing a nursing care plan is data collection, also known as assessment. This involves gathering comprehensive information about the patient’s health status using various techniques:
- Physical Assessment: A systematic examination of the patient’s body to identify physical signs and symptoms.
- Health History: Obtaining a detailed account of the patient’s past and present health conditions, including medical history, surgical history, allergies, and medications.
- Interview: Directly questioning the patient and/or family members to gather subjective data about their health concerns, symptoms, and perceptions.
- Medical Records Review: Examining the patient’s medical chart for relevant information, including previous diagnoses, treatments, lab results, and progress notes.
- Diagnostic Studies: Reviewing results from laboratory tests, imaging studies, and other diagnostic procedures.
The culmination of this step is creating a client database, a comprehensive collection of all health-related information gathered. During assessment, nurses utilize critical thinking to identify relevant data, recognize patterns, and pinpoint potential health problems or risks. This process is crucial for accurate diagnosis and effective intervention planning. Some healthcare agencies or educational institutions may provide specific assessment formats to guide data collection.
Step 2: Data Analysis and Organization
Once comprehensive data is collected, the next step is data analysis and organization. This involves:
- Analyzing Data: Examining the collected data to identify significant patterns, trends, and deviations from normal health parameters.
- Clustering Data: Grouping related pieces of data together to identify potential problem areas. This helps to synthesize information and see connections that might not be apparent when looking at isolated data points.
- Organizing Data: Structuring the data logically, often using frameworks like body systems or functional health patterns, to facilitate the identification of nursing diagnoses and priorities.
This step is crucial for transitioning from raw data to meaningful clinical insights that will inform the subsequent steps of diagnosis and intervention planning.
Step 3: Formulating Nursing Diagnoses
Nursing diagnoses are the core of the nursing care plan, providing a standardized way to identify and address patient needs. They are clinical judgments about a patient’s responses to actual or potential health problems that nurses are qualified and licensed to treat. Nursing diagnoses are distinct from medical diagnoses, which focus on disease processes. Instead, nursing diagnoses focus on the patient’s response to illness or health conditions.
For a detailed guide on formulating nursing diagnoses, refer to: Nursing Diagnosis (NDx): Complete Guide and List.
Nursing diagnoses are typically structured using a three-part statement (PES):
- Problem: The patient’s health problem or need, based on standardized diagnostic labels (e.g., Impaired Physical Mobility).
- Etiology: The related factors or causes of the problem (“related to” – e.g., related to postoperative pain).
- Signs and Symptoms: The defining characteristics or evidence of the problem (“as evidenced by” – e.g., as evidenced by reluctance to move and verbal report of pain).
Example: Impaired Physical Mobility related to postoperative pain as evidenced by reluctance to move and verbal report of pain.
Step 4: Setting Priorities
Setting priorities involves ranking nursing diagnoses in order of importance. This step ensures that the most critical patient needs are addressed first. Prioritization is a dynamic process that may change as the patient’s condition evolves. Diagnoses are often categorized as high, medium, or low priority:
- High Priority: Life-threatening problems that require immediate intervention (e.g., Ineffective Airway Clearance).
- Medium Priority: Problems that are not directly life-threatening but may cause significant discomfort or complications if not addressed (e.g., Acute Pain).
- Low Priority: Problems that are related to the patient’s long-term well-being or coping (e.g., Deficient Knowledge).
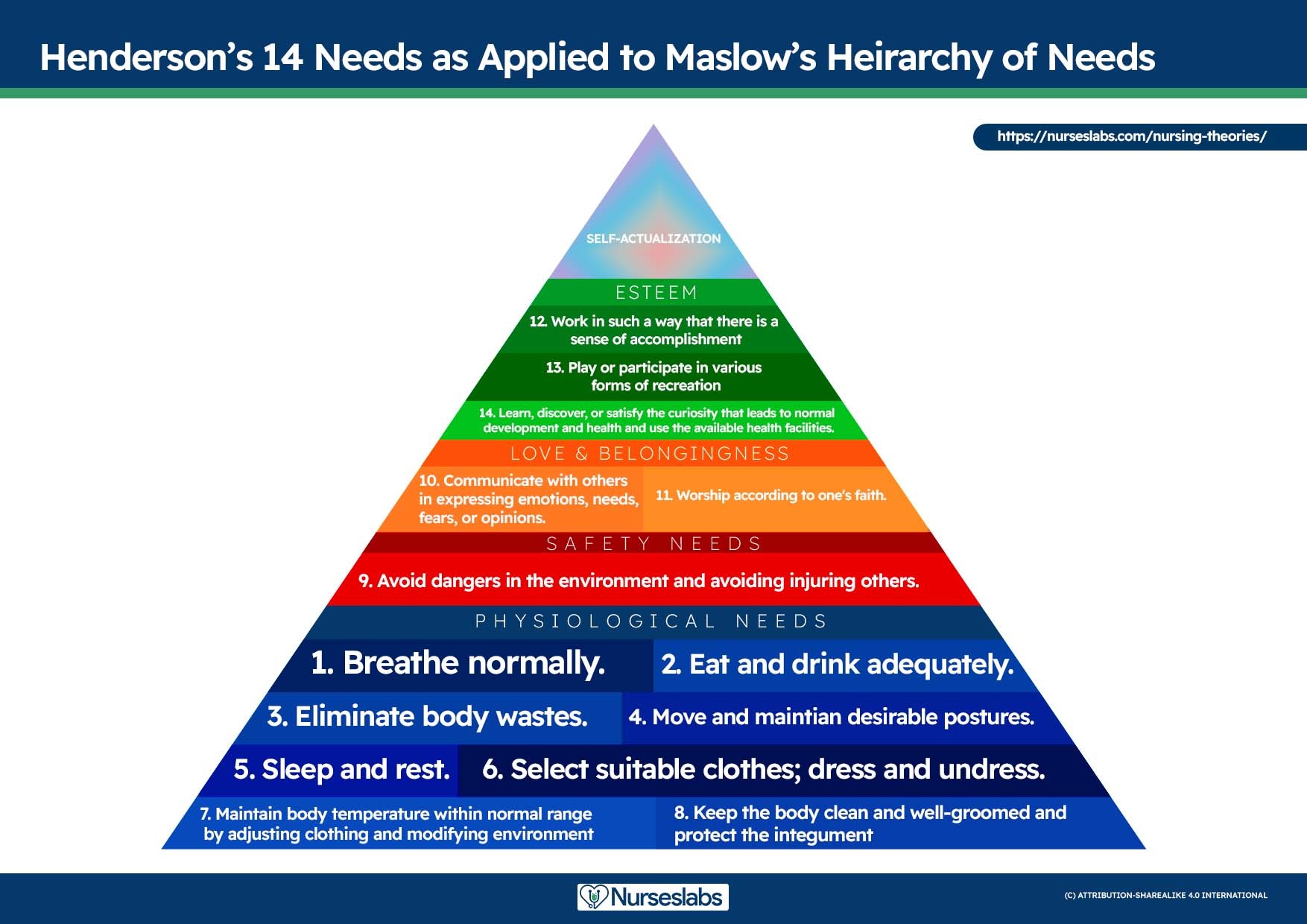
Maslow’s Hierarchy of Needs is a useful framework for setting priorities. This theory organizes human needs into a pyramid, with basic physiological needs at the base and higher-level needs at the top. According to Maslow, basic needs must be met before higher-level needs can be addressed.
Maslow’s Hierarchy of Needs in Nursing:
- Physiological Needs: Basic survival needs (e.g., airway, breathing, circulation, nutrition, elimination, sleep, pain relief).
- Safety and Security Needs: Needs for physical and emotional safety, security, and stability (e.g., fall prevention, infection control, safe environment).
- Love and Belonging Needs: Needs for social connection, intimacy, and belonging (e.g., fostering relationships, addressing social isolation).
- Self-Esteem Needs: Needs for confidence, achievement, respect, and independence (e.g., promoting self-efficacy, recognizing accomplishments).
- Self-Actualization Needs: Needs for personal growth, fulfillment, and achieving one’s full potential (e.g., supporting spiritual growth, empowering environment).
*Virginia Henderson’s 14 Needs as applied to Maslow’s Hierarchy of Needs. Learn more about it here. *
Factors to consider when setting priorities include the patient’s health values, beliefs, available resources, and the urgency of the problem. Involving the patient in this process is crucial for enhancing cooperation and ensuring the care plan aligns with their priorities.
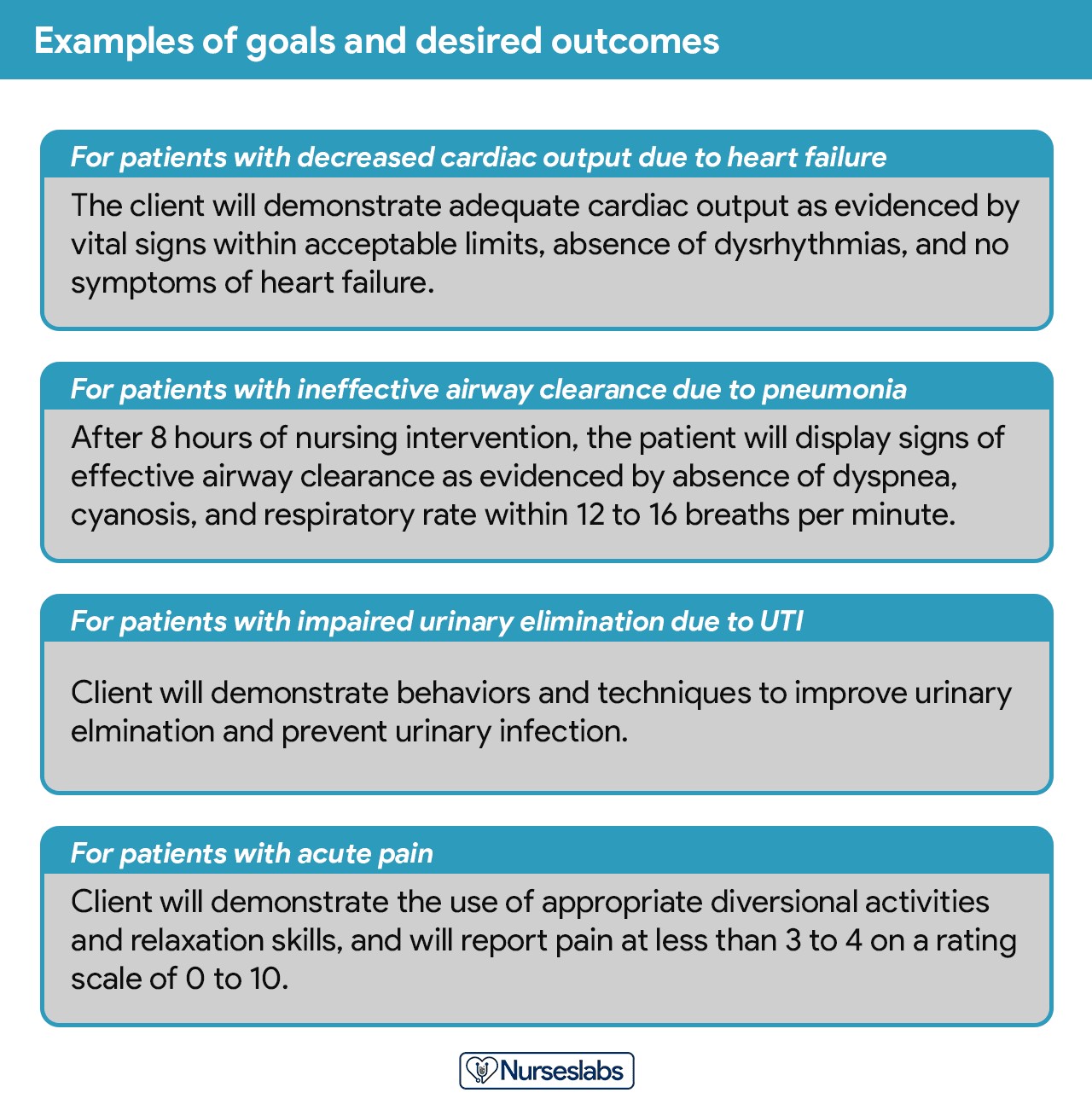
Step 5: Establishing Client Goals and Desired Outcomes
After prioritizing nursing diagnoses, the next step is to establish client goals and desired outcomes. Goals describe the broad, overall changes the nurse hopes to achieve, while desired outcomes are specific, measurable criteria that demonstrate goal attainment. Goals and outcomes are patient-centered and should reflect what the patient will achieve, not what the nurse will do.
Examples of goals and desired outcomes.
Goals should be SMART:
- Specific: Clearly defined and focused.
- Measurable: Quantifiable and able to be assessed.
- Attainable: Realistic and achievable for the patient.
- Relevant: Meaningful and important to the patient’s needs and values.
- Time-bound: Having a specific timeframe for achievement.
Outcomes should be written in observable and measurable terms, using action verbs that describe what the patient will do or demonstrate. Avoid vague terms like “improve” or “increase.”
Examples of SMART Outcomes:
- Short-term: “Patient will report pain level of 3 or less on a 0-10 scale within 1 hour after pain medication administration.”
- Long-term: “Patient will independently perform activities of daily living (ADLs) within 2 weeks of discharge.”
Goals can be classified as short-term or long-term:
- Short-term goals: Achievable within hours or days, often focused on immediate needs.
- Long-term goals: Achievable over weeks or months, typically related to rehabilitation or chronic conditions.
Desired outcome statements generally have four components:
- Subject: The patient (often implied).
- Verb: An action verb describing the desired patient behavior (e.g., “verbalize,” “demonstrate,” “walk”).
- Conditions or Modifiers: Specify the circumstances under which the behavior will occur (e.g., “using crutches,” “without assistance”).
- Criterion of Desired Performance: The standard for evaluating performance (e.g., “pain-free,” “for 50 feet”).
REEPIG Standards for High-Quality Goals:
- Realistic: Achievable with available resources.
- Explicitly Stated: Clear and unambiguous.
- Evidence-Based: Supported by research or best practices.
- Prioritized: Addressing the most urgent needs first.
- Involve Patient: Collaborative and patient-centered.
- Goal-Centered: Directly related to the nursing diagnosis.
Step 6: Selecting Nursing Interventions
Nursing interventions are the specific actions that nurses will implement to help the patient achieve the desired outcomes. Interventions should be evidence-based, tailored to the individual patient, and focused on addressing the etiology of the nursing diagnosis. For risk diagnoses, interventions should aim to reduce risk factors.
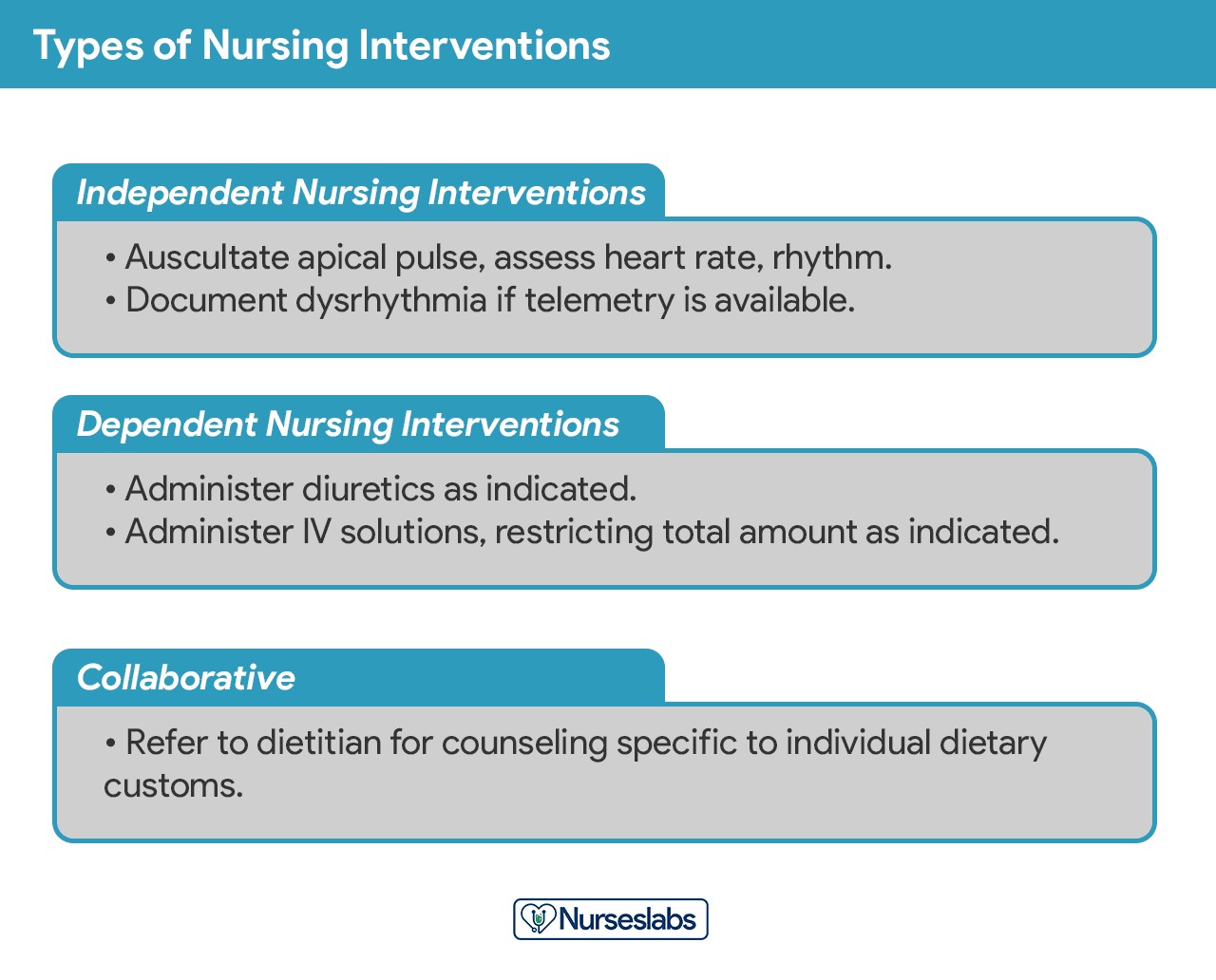
Types of nursing interventions in a care plan.
Types of Nursing Interventions:
- Independent Interventions: Actions that nurses are licensed to initiate based on their own judgment and skills (e.g., patient education, emotional support, positioning).
- Dependent Interventions: Actions that require a physician’s order (e.g., medication administration, intravenous therapy, specific treatments).
- Collaborative Interventions: Actions that require consultation or collaboration with other healthcare team members (e.g., physical therapy, dietary consult, social work referral).
Nursing interventions should be:
- Safe and Appropriate: Suitable for the patient’s age, health condition, and overall status.
- Achievable: Feasible with available resources and time.
- Patient-Centered: Aligned with the patient’s values, culture, and beliefs.
- Compatible with Other Therapies: Integrated with other aspects of the patient’s treatment plan.
- Evidence-Based: Supported by nursing knowledge, research, or relevant scientific principles.
When writing nursing interventions:
- Date and Sign: Document the date the plan is written and sign to indicate accountability.
- Specific and Clear: Use action verbs to start each intervention, specifying what, how, when, where, and how often the intervention should be performed.
- Use Accepted Abbreviations: Only use abbreviations approved by the healthcare institution.
Example: “Administer pain medication (morphine 2mg IV) every 4 hours PRN for pain rated >3 on a 0-10 scale.“
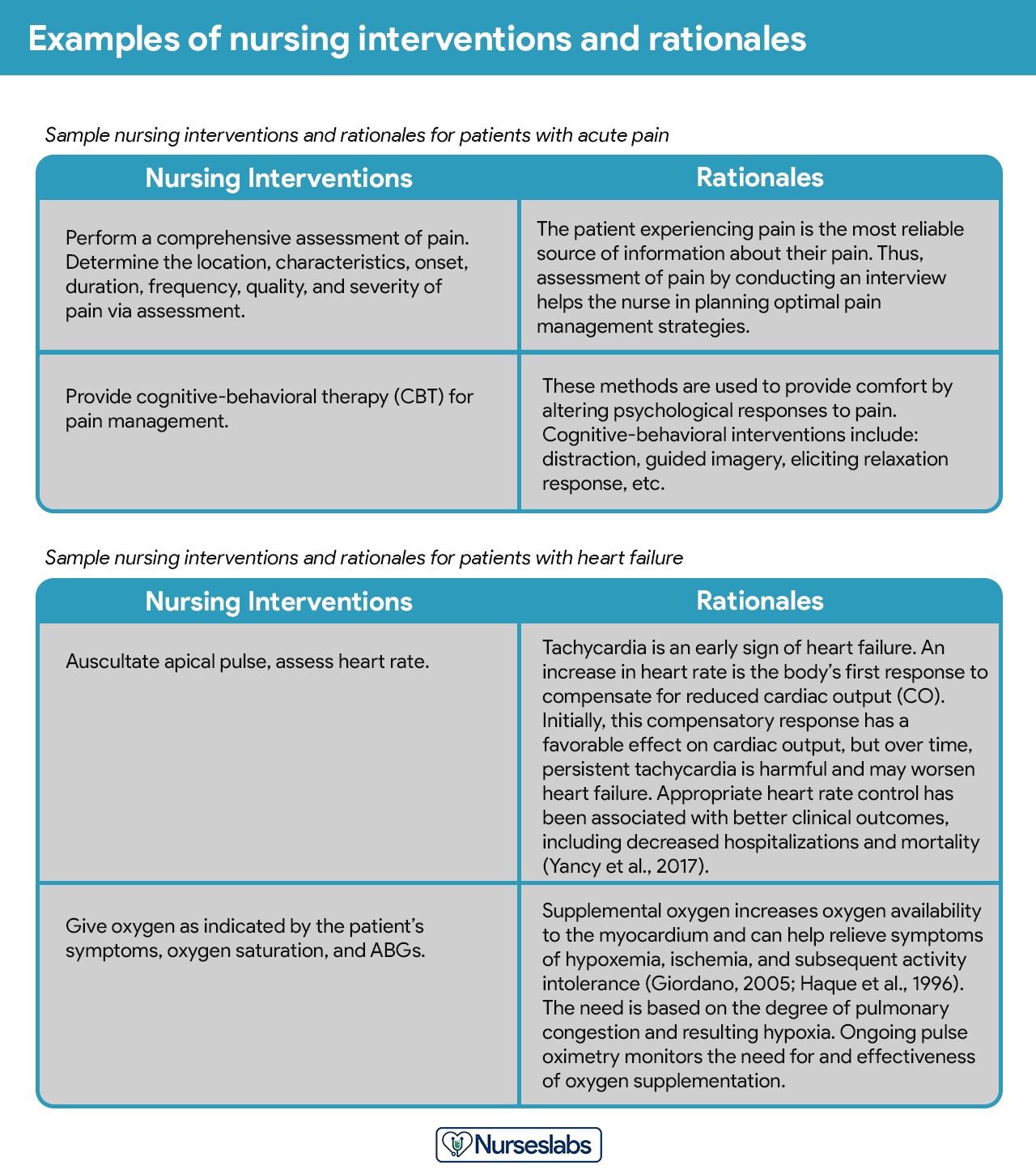
Step 7: Providing Rationale
Rationales, also known as scientific explanations, justify the selection of specific nursing interventions. They explain why an intervention is expected to be effective in achieving the desired outcome. Rationales are particularly important in student care plans to demonstrate understanding of the scientific principles underlying nursing care.
Example:
- Intervention: “Elevate the patient’s legs when in bed or chair.”
- Rationale: “Elevation promotes venous return and reduces edema in the lower extremities by utilizing gravity.”
Step 8: Evaluation
Evaluation is the final step of the nursing process, and it is an ongoing, planned activity. It involves assessing the patient’s progress towards achieving the desired outcomes and determining the effectiveness of the nursing care plan. Evaluation is crucial for determining whether the interventions should be continued, modified, or discontinued.
During evaluation, the nurse compares the patient’s current status to the desired outcomes established in Step 5. This involves:
- Collecting Re-assessment Data: Gathering new data to assess the patient’s current condition and response to interventions.
- Comparing Data to Outcomes: Analyzing the re-assessment data to determine if the desired outcomes have been met.
- Drawing Conclusions: Making judgments about the patient’s progress and the effectiveness of the care plan.
- Modifying the Care Plan (if needed): Adjusting the care plan based on the evaluation findings. This may involve revising nursing diagnoses, outcomes, or interventions.
Possible evaluation conclusions:
- Goal Met: The patient has achieved the desired outcome. Interventions may be discontinued for this specific outcome.
- Goal Partially Met: The patient has made some progress but has not fully achieved the outcome. Interventions may need to be continued and/or revised.
- Goal Not Met: The patient has made little or no progress towards the outcome. The care plan needs to be reassessed and significantly revised.
Step 9: Putting it on Paper (Documentation)
The final step is documenting the nursing care plan in the patient’s medical record. Documentation should be clear, concise, and accurate, following hospital policy and using the chosen care plan format. The care plan becomes a permanent part of the patient’s record and serves as a communication tool for all healthcare providers.
Nursing Care Plan List
This section provides a categorized list of sample nursing care plans (NCPs) and nursing diagnoses for various health conditions. These standardized care plans can serve as valuable frameworks for developing individualized plans.
Basic Nursing and General Care Plans
| Basic Nursing & General Care Plans |
|---|
| Acute Confusion (Delirium) and Altered Mental Status |
| Acute Pain and Pain Management |
| Activity Intolerance and Generalized Weakness |
| Cancer (Oncology Nursing) |
| Caregiver Role Strain and Family Caregiver Support Systems |
| Chronic Confusion (Dementia) |
| End-of-Life Care (Hospice Care or Palliative) |
| Fall Risk and Fall Prevention |
| Fatigue and Lethargy |
| Geriatric Nursing (Older Adult) |
| Grieving and Loss |
| Hypothermia and Cold Injuries |
| Hyperthermia (Fever) |
| Impaired Swallowing (Dysphagia) |
| Insomnia and Sleep Deprivation |
| Prolonged Bed Rest |
| Risk for Injury and Patient Safety |
| Self-Care and Activities of Daily Living (ADLs) |
| Surgery (Perioperative Client) |
| Systemic Lupus Erythematosus |
| Total Parenteral Nutrition |

Surgery and Perioperative Care Plans
| Surgery and Perioperative Care Plans |
|---|
| Amputation |
| Appendectomy |
| Cholecystectomy |
| Fracture UPDATED! |
| Hemorrhoids |
| Hysterectomy |
| Ileostomy & Colostomy |
| Laminectomy (Disc Surgery) |
| Mastectomy |
| Subtotal Gastrectomy |
| Surgery (Perioperative Client) |
| Thyroidectomy |
| Total Joint (Knee, Hip) Replacement |
Cardiac Care Plans
| Cardiac Care Plans |
|---|
| Angina Pectoris (Coronary Artery Disease) |
| Cardiac Arrhythmia (Digitalis Toxicity) |
| Cardiac Catheterization |
| Cardiogenic Shock |
| Congenital Heart Disease |
| Decreased Cardiac Output & Cardiac Support |
| Heart Failure UPDATED! |
| Hypertension UPDATED! |
| Hypovolemic Shock |
| Impaired Tissue Perfusion & Ischemia |
| Myocardial Infarction |
| Pacemaker Therapy |
Endocrine and Metabolic Care Plans
| Endocrine and Metabolic Care Plans |
|---|
| Addison’s Disease |
| Cushing’s Disease |
| Diabetes Mellitus (Type 1, Type 2) UPDATED! |
| Diabetic Ketoacidosis (DKA) and Hyperglycemic Hyperosmolar Nonketotic Syndrome (HHNS) |
| Eating Disorders: Anorexia & Bulimia Nervosa |
| Fluid Volume Deficit (Dehydration & Hypovolemia) |
| Fluid Volume Excess (Hypervolemia) |
| Gestational Diabetes Mellitus |
| Hyperthyroidism |
| Hypothyroidism |
| Imbalanced Nutrition (Malnutrition) |
| Obesity & Overweight |
| Thyroidectomy |
| Unstable Blood Glucose Levels (Hyperglycemia & Hypoglycemia) |
| Acid-Base Imbalances |
|---|
| Metabolic Acidosis |
| Metabolic Alkalosis |
| Respiratory Acidosis |
| Respiratory Alkalosis |
| Electrolyte Imbalances |
|---|
| Calcium (Ca) Imbalances: Hypercalcemia and Hypocalcemia |
| Magnesium (Mg) Imbalances: Hypermagnesemia and Hypomagnesemia |
| Potassium (K) Imbalances: Hyperkalemia and Hypokalemia |
| Sodium (Na) Imbalances: Hypernatremia and Hyponatremia |
Gastrointestinal Care Plans
| Gastrointestinal Care Plans |
|---|
| Appendectomy |
| Bowel Incontinence (Fecal Incontinence) |
| Cholecystectomy |
| Constipation |
| Diarrhea Nursing Care Plan and Management |
| Cholecystitis and Cholelithiasis |
| Gastroenteritis |
| Gastroesophageal Reflux Disease (GERD) |
| Hemorrhoids |
| Hepatitis |
| Ileostomy & Colostomy |
| Inflammatory Bowel Disease (IBD) |
| Intussusception |
| Liver Cirrhosis |
| Nausea & Vomiting |
| Pancreatitis |
| Peritonitis |
| Peptic Ulcer Disease |
| Subtotal Gastrectomy |
| Umbilical and Inguinal Hernia |
Hematologic and Lymphatic Care Plans
| Hematologic & Lymphatic Care Plans |
|---|
| Anaphylactic Shock |
| Anemia UPDATED! |
| Aortic Aneurysm |
| Bleeding Risk & Hemophilia |
| Deep Vein Thrombosis |
| Disseminated Intravascular Coagulation |
| Hemophilia |
| Kawasaki Disease |
| Leukemia |
| Lymphoma |
| Sepsis and Septicemia |
| Sickle Cell Anemia Crisis |
Infectious Diseases Care Plans
| Infectious Diseases Care Plans |
|---|
| Acquired Immunodeficiency Syndrome (AIDS) (HIV Positive) |
| Acute Rheumatic Fever |
| Dengue Hemorrhagic Fever |
| Herpes Zoster (Shingles) |
| Influenza (Flu) |
| Pulmonary Tuberculosis |
| Risk for Infection & Infection Control |
Integumentary Care Plans
| Integumentary Care Plans |
|---|
| Burn Injury |
| Dermatitis |
| Herpes Zoster (Shingles) |
| Pressure Ulcer (Bedsores) |
| Wound Care and Skin/Tissue Integrity |
Maternal and Newborn Care Plans
| Maternal and Newborn Care Plans |
|---|
| Abortion (Termination of Pregnancy) |
| Cervical Insufficiency (Premature Dilation of the Cervix) |
| Cesarean Birth |
| Cleft Palate and Cleft Lip |
| Gestational Diabetes Mellitus |
| Hyperbilirubinemia (Jaundice) |
| Labor Stages, Induced, Augmented, Dysfunctional, Precipitous Labor |
| Neonatal Sepsis |
| Perinatal Loss (Miscarriage, Stillbirth) |
| Placental Abruption |
| Placenta Previa |
| Postpartum Hemorrhage |
| Postpartum Thrombophlebitis |
| Prenatal Hemorrhage |
| Preeclampsia and Gestational Hypertension |
| Prenatal Infection |
| Preterm Labor |
| Puerperal & Postpartum Infections |
| Substance (Alcohol and Drug) Abuse in Pregnancy |
Mental Health and Psychiatric Care Plans
| Mental Health and Psychiatric Care Plans |
|---|
| Alcohol Withdrawal |
| Anxiety & Fear |
| Anxiety and Panic Disorders |
| Bipolar Disorders |
| Body Image Disturbance & Self-Esteem |
| Impaired Thought Processes & Cognitive Impairment |
| Major Depression |
| Personality Disorders |
| Schizophrenia |
| Sexual Assault |
| Substance Dependence and Abuse |
| Suicide Behaviors |
Musculoskeletal Care Plans
| Musculoskeletal Care Plans |
|---|
| Amputation |
| Congenital Hip Dysplasia |
| Fracture UPDATED! |
| Impaired Physical Mobility & Immobility |
| Juvenile Rheumatoid Arthritis |
| Laminectomy (Disc Surgery) |
| Osteoarthritis |
| Osteogenic Sarcoma (Osteosarcoma) |
| Osteoporosis |
| Rheumatoid Arthritis |
| Scoliosis |
| Spinal Cord Injury |
| Total Joint (Knee, Hip) Replacement |
Neurological Care Plans
| Neurological Care Plans |
|---|
| Alzheimer’s Disease UPDATED! |
| Brain Tumor |
| Cerebral Palsy |
| Cerebrovascular Accident (Stroke) UPDATED! |
| Guillain-Barre Syndrome |
| Meningitis |
| Multiple Sclerosis |
| Parkinson’s Disease |
| Seizure Disorder |
| Spinal Cord Injury |
Ophthalmic Care Plans
| Ophthalmic Care Plans |
|---|
| Cataracts |
| Glaucoma |
| Macular Degeneration |
Pediatric Nursing Care Plans
| Pediatric Nursing Care Plans |
|---|
| Child Abuse |
| Cleft Lip and Cleft Palate |
| Dying Child |
| Febrile Seizure |
| Hospitalized Child |
| Hydrocephalus |
| Otitis Media |
| Spina Bifida |
| Tonsillitis and Adenoiditis |
Reproductive Care Plans
| Reproductive Care Plans |
|---|
| Cryptorchidism (Undescended Testes) |
| Hysterectomy |
| Hypospadias and Epispadias |
| Mastectomy |
| Menopause |
| Prostatectomy |
Respiratory Care Plans
| Respiratory Care Plans |
|---|
| Airway Clearance Therapy & Coughing |
| Apnea |
| Asthma UPDATED! |
| Aspiration Risk & Aspiration Pneumonia |
| Bronchiolitis UPDATED! |
| Bronchopulmonary Dysplasia (BPD) UPDATED! |
| Chronic Obstructive Pulmonary Disease (COPD) UPDATED! |
| Croup Syndrome |
| Cystic Fibrosis UPDATED! |
| Epiglottitis |
| Hemothorax and Pneumothorax UPDATED! |
| Ineffective Breathing Pattern (Dyspnea) |
| Impairment of Gas Exchange |
| Influenza (Flu) UPDATED! |
| Lung Cancer UPDATED! |
| Mechanical Ventilation |
| Near-Drowning |
| Pleural Effusion |
| Pneumonia |
| Pulmonary Embolism |
| Pulmonary Tuberculosis |
| Tracheostomy |
Urinary Care Plans
| Urinary Care Plans |
|---|
| Acute Glomerulonephritis |
| Acute Renal Failure |
| Benign Prostatic Hyperplasia (BPH) |
| Chronic Renal Failure |
| Hemodialysis |
| Nephrotic Syndrome |
| Peritoneal Dialysis |
| Urolithiasis (Renal Calculi) |
| Urinary Elimination (Urinary Incontinence & Urinary Retention) |
| Urinary Tract Infection |
| Vesicoureteral Reflux (VUR) |
| Wilms Tumor (Nephroblastoma) |
Recommended Resources
Enhance your nursing care planning skills with these recommended resources:
Disclosure: The following are affiliate links from Amazon.com. We may earn a small commission from your purchase at no additional cost to you.
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition)
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care
All-in-One Nursing Care Planning Resource – E-Book: Medical-Surgical, Pediatric, Maternity, and Psychiatric-Mental Health
By mastering the principles and steps outlined in this guide, nurses can develop effective nursing care plans that drive positive patient outcomes and contribute to excellence in healthcare.