Introduction
Autoimmune hemolytic anemia (AIHA) is a condition characterized by the immune system mistakenly attacking and destroying the body’s own red blood cells. As experts in automotive diagnostics at xentrydiagnosis.store, while our primary focus is vehicle repair, understanding complex diagnostic approaches is fundamental to our problem-solving skillset. In the medical field, diagnosing AIHA requires a meticulous, stepwise approach, much like diagnosing intricate automotive issues. This article will delve into the differential diagnosis of AIHA, a critical aspect for healthcare professionals, mirroring the systematic diagnostic thinking we apply to vehicles. Just as we differentiate between electrical, mechanical, or sensor-related problems in cars, clinicians must distinguish AIHA from other causes of anemia and hemolysis. This detailed guide aims to provide a comprehensive understanding of the AIHA differential diagnosis, mirroring our commitment to in-depth diagnostic knowledge.
Understanding the Diagnostic Approach to Autoimmune Hemolytic Anemia
When a patient presents with anemia, the initial diagnostic step is to confirm hemolysis – the destruction of red blood cells. This process is akin to identifying a fault in a car system before pinpointing the exact component. The diagnostic pathway for AIHA is a process of exclusion, much like ruling out possible causes in a vehicle malfunction. We start with basic investigations to suggest hemolysis and then move towards confirming its autoimmune nature.
Initial Investigations for Hemolysis
Similar to using basic OBD-II scans and visual inspections in automotive repair, initial investigations for hemolysis are relatively straightforward. These tests, summarized in Table 1, are not solely specific to AIHA but are indicative of hemolytic processes.
Table 1. Initial Diagnostic Tests for Hemolysis
| Diagnostic Test | Indication for Hemolysis | Automotive Diagnostic Analogy |
|---|---|---|
| Complete Blood Count (CBC) | Anemia (Normo/Macrocytic) | Checking fluid levels (engine oil, coolant) – low levels signal a problem |
| Reticulocyte Count | Elevated | Observing engine RPM response – high revving might indicate issue |
| Unconjugated Bilirubin | Elevated | Checking exhaust for unusual emissions – byproducts indicate issue |
| Haptoglobin | Reduced | Assessing fluid leaks – loss of fluid indicates a problem |
| Blood Smear | Polychromasia, Spherocytes, Agglutination | Visual inspection of components – unusual appearance suggests issue |
| Lactate Dehydrogenase (LDH) | Elevated | Measuring system voltage – high voltage might indicate issue |
These initial tests are analogous to preliminary checks in automotive repair. For instance, a normo- or macrocytic anemia is like noticing low fluid levels in a vehicle, suggesting a system issue. An elevated reticulocyte count, indicating the bone marrow’s attempt to compensate for red cell loss, is similar to an engine revving high to compensate for a problem. Raised unconjugated bilirubin, a byproduct of heme breakdown, is akin to unusual emissions from a vehicle, signaling an abnormal process. Reduced haptoglobin, a protein that binds free hemoglobin, is like noticing fluid leaks, indicating loss of system components. Blood smear findings like polychromasia (immature red blood cells), spherocytes (球形红细胞), or agglutination (clumping of red cells) are comparable to visual inspections revealing damaged or abnormal parts. Elevated LDH, released from damaged cells, is similar to high voltage readings, suggesting system stress or damage.
However, just as individual automotive tests can be non-specific, these hematological tests also have limitations. Elevated LDH and reduced haptoglobin can occur in liver disease, similar to how electrical issues can mimic mechanical problems in a car. Bilirubin may be normal in mild hemolysis, like subtle car issues being hard to detect initially. Spherocytes are not always visible, and reticulocytopenia (low reticulocyte count) can occur in AIHA, especially if the bone marrow is infiltrated by disorders or suppressed by infections like parvovirus B19. This is akin to a car’s computer masking the true issue. Intravascular hemolysis, suggested by significantly raised LDH, red cell fragments on smear, or urinary hemosiderin, points to more specific causes, similar to identifying a major component failure in a vehicle.
Table 2. Causes of Intravascular Hemolysis
| Cause Category | Examples | Automotive Analogy |
|---|---|---|
| Complement Fixation | Paroxysmal nocturnal hemoglobinuria, Paroxysmal cold hemoglobinuria, Mismatched blood transfusion, Complement-mediated AIHA | Systemic fluid contamination causing internal damage |
| Mechanical Trauma | Cardiac valves, Microthrombi (DIC, MAHA – TTP, HUS, aHUS), March hemoglobinuria | Physical damage to components due to faulty parts or obstruction |
| Toxic/Exogenous Factors | Infections (Babesia, Clostridium, Leptospira, Falciparum malaria), Spider bites, Snake venoms, Copper/zinc toxicity, Hypotonic solutions | External contamination or incorrect fluids causing system failure |
Just as identifying intravascular hemolysis narrows down the possibilities, recognizing specific symptoms in a car can quickly point towards certain systems. For example, complement fixation-related intravascular hemolysis is like systemic fluid contamination, affecting multiple areas. Mechanical trauma-induced hemolysis is akin to physical damage from component failure or obstruction. Toxic or exogenous factors are comparable to external contamination or using incorrect fluids, leading to system malfunction.
Confirming Immune Hemolysis: The Direct Antiglobulin Test (DAT)
Once hemolysis is confirmed, the next crucial step is to determine if it’s immune-mediated. This is where the Direct Antiglobulin Test (DAT), also known as Coombs test, comes into play, the cornerstone of AIHA diagnosis. The DAT detects antibodies (IgG, IgM, IgA) or complement proteins (C3d) bound to the red blood cell surface. A positive DAT strongly suggests autoimmune hemolysis, analogous to a positive diagnostic scan confirming a specific system fault in a car.
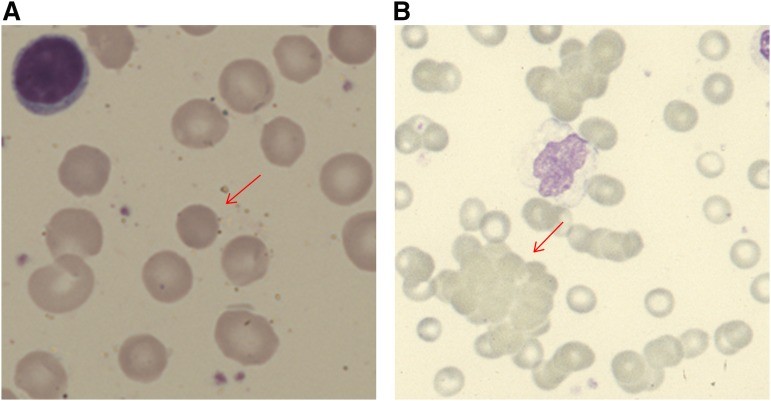
Figure 1. Blood film appearances in patients with AIHA.
(A) Spherocyte in a patient with warm AIHA (original magnification, ×100). (B) Red cell agglutination in a patient with cold agglutinin disease (×40).
Alt text: Microscopic blood smear images illustrating key features of Autoimmune Hemolytic Anemia (AIHA). Image A displays a spherocyte, a characteristic red blood cell in warm AIHA, magnified 100 times. Image B shows red cell agglutination, clumping of red blood cells typical in cold agglutinin disease, magnified 40 times.
However, a positive DAT is not exclusive to AIHA. Similar to how a diagnostic code might indicate a sensor issue but the root cause could be wiring, other conditions can cause a positive DAT. These include:
- Recent Blood Transfusion: Delayed transfusion reactions can cause a positive DAT, just as incorrect fluid top-up in a car can cause issues.
- Alloimmune Hemolysis: Post-transplant or hemolytic disease of the newborn, analogous to system incompatibility after part replacement.
- Drug-Induced Immune Hemolysis: Certain drugs can trigger a positive DAT, similar to aftermarket parts causing system conflicts.
- Passive Antibody Deposition: Liver disease, chronic infections, malignancies, SLE, renal disorders, and IV Ig or anti-thymocyte globulin therapies can cause non-AIHA positive DAT, comparable to external factors affecting car systems without direct component failure.
Therefore, the differential diagnosis must exclude these alternative causes of a positive DAT. Just as we rule out external factors or recent modifications in car diagnostics, clinicians must consider these factors.
DAT-Negative AIHA
In rare instances, AIHA can be DAT-negative. This is analogous to intermittent car problems that don’t trigger diagnostic codes immediately. DAT-negative AIHA may be due to low-affinity antibodies or IgA-only antibodies, which standard DAT may miss. Diagnosis relies on:
- Exclusion of other hemolysis causes: Ruling out all other potential issues, similar to comprehensive car diagnostics.
- Sensitive techniques: Specialized lab tests to detect subtle immune markers, like advanced diagnostic tools for elusive car faults.
- Response to steroids: Therapeutic response to steroids can support the diagnosis, similar to observing improvement after a suspected component is addressed in a car.
Differential Diagnosis of AIHA Subtypes and Associated Conditions
Once AIHA is diagnosed, differentiating between its subtypes and identifying underlying conditions is crucial. This step is akin to identifying the specific system and component within a car that is causing the problem. The AIHA subtypes – warm AIHA, cold agglutinin disease (CAD), mixed AIHA, and paroxysmal cold hemoglobinuria (PCH) – each have distinct characteristics and require different management strategies.
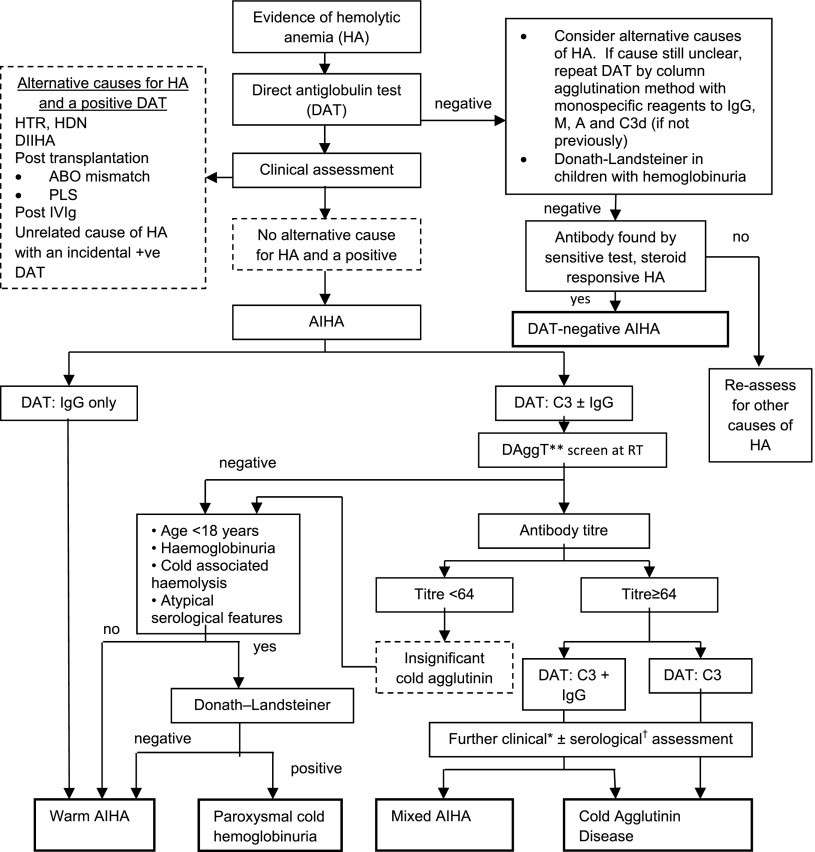
Figure 2. Diagnostic pathway for AIHA.
Alt text: Flowchart illustrating a diagnostic pathway for Autoimmune Hemolytic Anemia (AIHA). The chart begins with ‘Suspect Hemolysis,’ progresses through key tests like DAT, DAggT, and Cold Antibody Titer, and differentiates between subtypes including Warm AIHA, Cold Agglutinin Disease (CAD), Mixed AIHA, Drug-Induced Immune Hemolytic Anemia (DIIHA), and Paroxysmal Cold Hemoglobinuria (PCH). It emphasizes clinical picture synthesis and specialist lab advice for final diagnosis.
Table 3. Differential Diagnosis of AIHA Subtypes
| AIHA Subtype | Key Diagnostic Features