Heart failure (HF) is a significant global health concern, recognized as a major contributor to cardiovascular morbidity and mortality. Diagnosing heart failure accurately is crucial for timely and effective management, yet it often presents a clinical challenge. While the diagnostic process traditionally relies on patient history, physical examinations, and chest X-ray findings, these methods alone can be insufficient. Many conditions affecting the cardiopulmonary system can mimic heart failure symptoms, leading to diagnostic uncertainty and delays in appropriate treatment. In such scenarios, biomarkers that can reliably pinpoint heart failure as the underlying cause of a patient’s symptoms are invaluable for guiding prompt and effective intervention.
B-type natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP) have emerged as such critical biomarkers. These natriuretic peptides are now widely utilized in both the diagnosis and management of heart failure. However, understanding their role in the Bnp Differential Diagnosis is essential for accurate clinical interpretation and patient care.
Understanding BNP and NT-proBNP
To effectively use BNP in differential diagnosis, it’s crucial to understand its origins, actions, and metabolism.
Chemistry and Synthesis
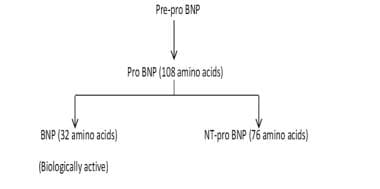
Natriuretic peptides are protein molecules secreted by the heart’s ventricles in response to increased volume or pressure. BNP, a 32-amino acid protein, originates from a larger precursor molecule called proBNP within the ventricular muscle cells. When the heart experiences volume or pressure overload, the ventricular muscle releases pre-proBNP. This is then cleaved into a 108-amino acid proBNP, which is further processed into two key components: biologically active BNP and the inert NT-proBNP (76 amino acids). This process is illustrated in the image below.
{kind=link}
Normal Actions
The primary function of natriuretic peptides is to assist the heart in managing volume overload and cardiac muscle stretch. BNP, being biologically active, promotes natriuresis (sodium excretion), vasodilation, and diuresis (fluid excretion). These actions collectively contribute to improved myocardial relaxation and counteract the effects of the renin-angiotensin-aldosterone system, a hormone system that regulates blood pressure and fluid balance. In contrast, NT-proBNP is biologically inactive.
It’s important to note that natriuretic peptides are primarily synthesized and released in response to ventricular stress, with minimal storage in granules. This means that in cases of acute heart failure decompensation, there may be a delay between the onset of clinical deterioration and a noticeable increase in natriuretic peptide levels.
Metabolism
The precise metabolic pathways of natriuretic peptides are complex and not fully understood. BNP is metabolized through several mechanisms, including neutral endopeptidases, natriuretic peptide receptor-C (NPR-C) mediated degradation, and, to a lesser extent, renal metabolism. NT-proBNP, on the other hand, undergoes greater renal clearance than BNP and is also cleared by other highly perfused organs like the liver and muscles.
Clinical Applications of BNP in Heart Failure Diagnosis
The most clinically significant application of BNP and NT-proBNP is in diagnosing heart failure as the cause of a patient’s symptoms, particularly when the diagnosis is uncertain. This is strongly supported by numerous evidence-based clinical guidelines. Early BNP testing in such situations can enhance diagnostic accuracy, ensure timely diagnosis, prevent treatment delays, reduce hospital stays, and lower healthcare costs. However, it’s crucial to remember that elevated natriuretic peptide levels alone should not definitively confirm or exclude heart failure as the cause of symptoms.
Beyond initial diagnosis, elevated BNP and NT-proBNP levels are observed in various other clinical contexts. While their use in many of these settings is still under investigation, their clinical utility is increasingly recognized.
BNP Differential Diagnosis: Factors Affecting BNP Levels
Interpreting BNP levels requires careful consideration of factors that can lead to falsely low or falsely high readings. This is critical for accurate BNP differential diagnosis.
Conditions Causing Falsely Low BNP
Several clinical conditions can result in deceptively low natriuretic peptide levels despite the presence of heart failure.
-
Obesity: Obese individuals often exhibit lower natriuretic peptide levels even with overt heart failure signs and symptoms. This phenomenon has been consistently observed in multiple studies. While the exact reasons remain unclear, BNP still retains prognostic value in obese patients, with higher levels correlating with poorer outcomes. While a lower BNP cutoff value has been suggested for obese patients, the specific value remains a subject of debate.
-
Flash Pulmonary Edema: In the initial 1-2 hours following the onset of flash pulmonary edema (sudden, severe fluid buildup in the lungs), BNP levels might be lower than expected. This is because natriuretic peptides are synthesized in response to acute ventricular pressure or volume overload, and there is limited pre-existing storage for immediate release during decompensation.
-
Heart Failure Due to Upstream Causes: When heart failure symptoms originate from issues upstream of the left ventricle, such as mitral regurgitation or mitral stenosis, BNP levels may only be mildly elevated despite significant heart failure symptoms. Similarly, patients with heart failure due to constrictive pericarditis (inflammation of the sac surrounding the heart) or restrictive cardiomyopathy (stiffening of the heart muscle) may present with significant heart failure symptoms but only modestly elevated BNP levels.
Conditions Causing Falsely High BNP
Conversely, falsely elevated BNP and NT-proBNP levels can be observed in certain populations.
- Age and Renal Function: Females, older individuals, and patients with renal failure (kidney dysfunction) may exhibit higher BNP and NT-proBNP levels. This is partly due to reduced renal clearance of NT-proBNP and age-related changes in cardiac function.
Gray Zone BNP Values and Age
A “gray zone” exists in BNP and NT-proBNP interpretation for heart failure diagnosis, particularly concerning age. As shown in Table 2, age-related reference ranges are important to consider.
| BNP | NT-proBNP |
|---|---|
| 100-400 pg/mL | 50-75 years – 300-900 pg/mL >75 years – 300-1800 pg/mL |
When natriuretic peptide values fall within these gray zones, a definitive heart failure diagnosis necessitates careful clinical evaluation and further confirmatory testing. Clinicians must also consider other conditions beyond congestive heart failure that can cause mild elevations in natriuretic peptide levels. It is important to note that BNP levels are elevated in both systolic heart failure (reduced ejection fraction) and heart failure with preserved ejection fraction (diastolic heart failure). BNP value alone cannot differentiate between these two types of heart failure.
Recent research, such as a study by Reynen et al., indicates that urinary NT-proBNP levels also hold cardiovascular significance, mirroring plasma levels in predicting all-cause mortality and major adverse cardiac events in patients with acute chest pain. Urinary and plasma NT-proBNP levels were found to be highest in patients with troponin-positive acute coronary syndrome and congestive heart failure.
Conclusion
BNP and NT-proBNP are invaluable tools in the diagnostic armamentarium for heart failure. However, their optimal use requires a nuanced understanding of factors influencing their levels. Effective BNP differential diagnosis necessitates considering patient-specific characteristics, potential conditions causing false readings, and age-adjusted reference ranges. While these biomarkers significantly enhance diagnostic accuracy and guide timely management, they should always be interpreted in conjunction with comprehensive clinical assessment and other diagnostic modalities to ensure optimal patient care.