Introduction
Symptoms related to laryngeal lesions are diverse, ranging from hoarseness and dysphagia to odynophagia, globus sensation, and breathing difficulties. Clinical guidelines emphasize the importance of referral to head and neck specialists for patients presenting with such symptoms, necessitating thorough evaluation, often including direct laryngoscopy. When an epiglottic lesion is identified, management strategies vary based on symptom severity and lesion size. While small, benign-appearing lesions may be monitored, masses with uncertain characteristics or those causing airway obstruction often require excision.
Cross-sectional imaging, particularly Computed Tomography (CT) and Magnetic Resonance Imaging (MRI), plays a crucial role in evaluating clinically suspicious or potentially malignant lesions, aiding in detailed characterization and assessing the extent of disease. Radiologists frequently encounter benign-appearing epiglottic masses as incidental findings during imaging performed for unrelated reasons or to investigate indeterminate physical exam results. In these scenarios, understanding the Broad Differential Diagnosis Meaning becomes paramount.
This article aims to equip radiologists with a comprehensive understanding of the broad spectrum of differential diagnoses for polypoid epiglottic masses. Using a case of benign squamous papilloma as a starting point, we will delve into the clinical presentations and imaging characteristics of various epiglottic masses. By providing insights into narrowing the differential diagnosis, we underscore the radiologist’s vital role in guiding clinical management.
Case Presentation: Benign Squamous Papilloma of the Epiglottis
A 65-year-old female presented to a gastroenterologist with a history of dyspepsia and heartburn spanning several months. Upper endoscopy revealed a non-bleeding gastric erosion, diagnosed as mild chronic gastritis via biopsy, and an unexpected medium-sized polypoid mass on the epiglottis. Subsequently, she was referred to an otolaryngologist for further evaluation. The patient reported no sore throat, swallowing difficulties, voice changes, or neck or ear pain. Her medical history included significant alcohol consumption and a 30-year history of smoking one pack of cigarettes daily, though she had quit smoking 12 years prior and reduced her alcohol intake. Fiberoptic laryngeal examination revealed a 1 cm exophytic, pedunculated, papillomatous lesion on the laryngeal surface of the suprahyoid epiglottis, near the midline. The initial clinical differential diagnosis included benign papilloma versus a well-differentiated, papillomatous-appearing laryngeal malignancy. Despite the benign appearance, the patient’s smoking history, a major risk factor for laryngeal cancer (with up to 95% of laryngeal cancer patients having a history of tobacco use), prompted a CT scan to rule out deeper invasion indicative of malignancy. The CT scan showed no malignant features, and the patient underwent excisional biopsy with a CO2 laser, revealing a benign squamous papilloma upon pathological examination. During surgery, the lesion appeared superficial, without apparent cartilaginous involvement (Figure 1).
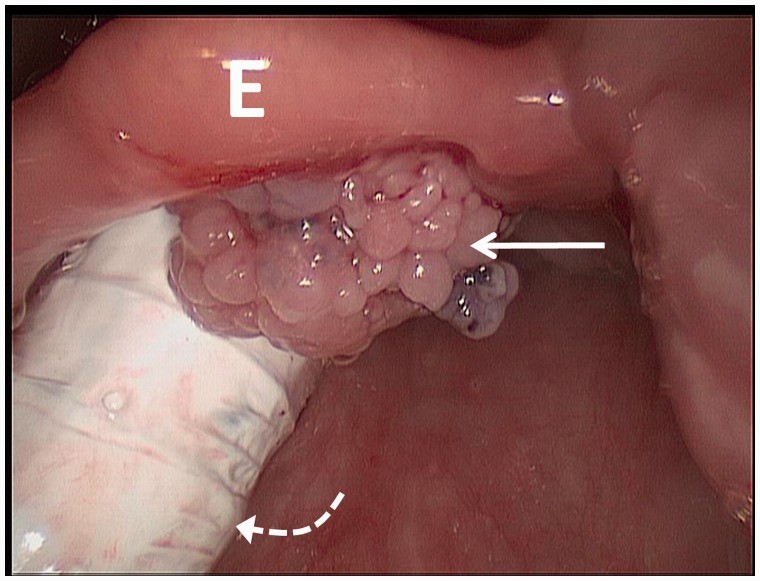
Figure 1. Intraoperative Laryngoscopy Image of Epiglottic Papilloma
Figure 1. Intra-operative laryngoscopy photograph showing an approximately 1 cm exophytic, pedunculated, papillomatous lesion (arrow) on the laryngeal surface of the suprahyoid epiglottis (E), close to midline, without apparent involvement of the underlying cartilage. The endotracheal tube is seen posteriorly (curved dotted arrow).
Imaging Findings: CT Characteristics of a Benign Epiglottic Lesion
The CT scan demonstrated a well-defined, 0.7 cm × 0.5 cm × 0.5 cm (transverse × anterior-posterior × craniocaudal) structure with a density of approximately 50 Hounsfield Units, attached to the posterior (laryngeal) surface of the right parasagittal epiglottis (Figure 2). Crucially, the epiglottis itself was not thickened, and the remaining supraglottic larynx, including aryepiglottic folds, false vocal cords, vestibule, pre-epiglottic and para-epiglottic spaces, and arytenoid cartilages, appeared normal. The glottic and subglottic larynx were also unremarkable.
Figure 2. Axial and Sagittal CT Images of Benign Epiglottic Mass
Figure 2. Axial (a) and sagittal (b) contrast-enhanced computed tomography (CT) images of a 65-year-old female patient showing a 0.7 cm × 0.5 cm × 0.5 cm circumscribed structure (arrow) of approximately 50 Hounsfield units, inseparable from the posterior (laryngeal) surface of the right parasagittal epiglottis. The epiglottis was not thickened, and the remainder of the larynx appeared normal.
Pathological Diagnosis: Benign Squamous Papilloma Confirmed
Histopathological examination of the excisional biopsy specimen, a papillary cauliflower-like tissue measuring 0.8 cm × 0.8 cm × 0.6 cm, revealed a benign lesion characterized by fibrovascular cores covered by mature keratinizing stratified squamous epithelium (Figure 3). There was no evidence of epithelial dysplasia, atypical mitosis, or invasion.
Figure 3. Microscopic View of Benign Squamous Papilloma
Figure 3. Low-power magnification showing central fibrovascular cores covered by benign keratinizing squamous epithelium.
Discussion: Navigating the Broad Differential Diagnosis of Epiglottic Masses
Epiglottic masses represent a diagnostic challenge due to their diverse etiologies, encompassing cystic, granulomatous, infectious, neoplastic, and systemic disease manifestations. The radiologist’s expertise is crucial in narrowing this broad differential diagnosis to guide appropriate patient management. While acute epiglottitis, a critical emergency, is often diagnosed clinically based on rapid onset stridor, dysphagia, high fever, and toxic appearance, our focus here is on the broader spectrum of epiglottic masses that may present with more subtle or incidental findings. We will not delve into conditions causing diffuse epiglottic thickening such as acute epiglottitis or radiation effects, unless they coexist with a discrete mass.
Benign Neoplastic and Non-Neoplastic Epiglottic Masses
Benign growths, both neoplastic and non-neoplastic, can manifest as epiglottic masses. Squamous papillomas, as seen in our case, are slow-growing, non-invasive epithelial tumors forming well-defined papillary masses, often pedunculated. While commonly found in the soft palate, tonsils, and pharyngeal wall, laryngeal involvement, including the epiglottis, is frequent and can be symptomatic. These lesions are characterized by exophytic papillary fronds covered by mature stratified squamous epithelium and are linked to Human Papillomavirus (HPV), which is also associated with an increased risk of laryngeal squamous cell carcinoma.
Fibroepithelial polyps, another benign entity, are similar to papillomas in their non-invasive nature but differ in composition, featuring a larger solid fibrous core rather than multiple fine papillae and lacking squamous epithelial overgrowth. On MRI, they typically exhibit T2 hyperintensity, mild T1 hyperintensity, and no enhancement post-gadolinium contrast.
Laryngeal cysts, predominantly ductal cysts, constitute a significant portion of benign laryngeal lesions, with the epiglottis being a common site. These cysts, visualized on CT as low-density structures, can become secondarily infected, mimicking epiglottitis with potential ring enhancement on contrast-enhanced CT. It’s crucial to differentiate abscess formation from normal air within an epiglottic cyst. Large epiglottic cysts can cause airway obstruction.
Uncommon benign tumors such as extracardiac rhabdomyomas, solitary fibrous tumors, neurogenic tumors (schwannomas, neurofibromas, malignant peripheral nerve sheath tumors), and hamartomas can also present as epiglottic masses. Schwannomas, though rare in the larynx, can occur on the epiglottis, presenting as pedunculated, smooth masses. Hamartomas, benign proliferations of epithelial and mesenchymal tissues, may appear as heterogeneous masses containing fat density on CT, often recurring post-excision due to ill-defined margins. Paragangliomas, though usually malignant in the larynx, are also part of the differential.
Granulomatous Diseases Affecting the Epiglottis
Granulomatous conditions like tuberculosis, sarcoidosis, and Wegener’s granulomatosis should be considered in the broad differential diagnosis meaning of epiglottic masses. Laryngeal sarcoidosis frequently involves the epiglottis, presenting with erythema, edema, nodules, and mass lesions. Laryngeal tuberculosis, while uncommon overall, rarely affects the epiglottis specifically, typically manifesting as thickening rather than a discrete mass. Epiglottic tuberculosis may present with thickened free margins and aryepiglottic fold thickening, often sparing the pre-epiglottic fat spaces, contrasting with laryngeal carcinoma which commonly infiltrates this space. While symptoms can overlap, hoarseness is more typical in tuberculosis, whereas foreign body sensation and referred otalgia are more common in carcinoma. Differentiating tuberculosis from carcinoma is crucial, and imaging signs of invasion like cartilaginous erosion or pre-epiglottic/paraglottic fat space involvement are important indicators of malignancy.
Infectious Etiologies of Epiglottic Masses
Infections such as histoplasmosis can also manifest as epiglottic masses. Laryngeal histoplasmosis, though more common in the anterior larynx and oropharynx, can involve the epiglottis, presenting as a mass with erosion.
Malignant Epiglottic Masses
While less common than benign lesions, malignant tumors must be considered in the broad differential diagnosis meaning. Squamous cell carcinoma is the most frequent laryngeal malignancy, although mucoepidermoid carcinoma, small cell carcinoma, lymphoma, and solitary plasmacytoma, and even metastatic lesions are also possible, albeit rare. Laryngeal lymphoma, typically of B-cell non-Hodgkin subtypes, often involves the supraglottic larynx, including the epiglottis, showing isointensity on T1- and T2-weighted MRI with homogeneous contrast enhancement. Solitary plasmacytoma can present as a submucosal epiglottic mass. Metastases to the larynx are exceedingly rare but reported.
Squamous cell carcinoma of the epiglottis, especially when small and midline, can mimic benign lesions, but often presents with bilateral lymphadenopathy (Figure 4).
Figure 4. CT Images of Malignant Epiglottic Mass (Squamous Cell Carcinoma)
Figure 4. Axial (a) and sagittal (b) contrast-enhanced computed tomography (CT) images of a 73-year-old male patient with foreign body sensation revealing a 2.6 cm × 1.5 cm × 2.0 cm epiglottic mass (arrow) of approximately 70 Hounsfield units biopsy proven squamous cell carcinoma. A necrotic lymph node was also identified (curved arrow).
Cartilaginous and Lymphatic Lesions of the Epiglottis
Given the epiglottis’s cartilaginous composition, cartilaginous tumors like chondromas and chondrosarcomas are relevant to the differential diagnosis. Chondromas of the epiglottis are rare, often presenting with calcifications and T2 hyperintensity on MRI. Distinguishing chondromas (typically <2 cm) from chondrosarcomas (>3 cm) can be challenging both radiologically and histologically. Laryngeal chondrosarcomas rarely involve the epiglottis.
Lymphangiomas (lymphatic malformations) are important to consider, particularly in pediatric cases, typically arising in the supraglottic larynx and appearing T2 hyperintense on MRI. While more common in children, they can also occur in adults.
Systemic Diseases Manifesting as Epiglottic Masses
Systemic conditions including systemic lupus erythematosus, rheumatoid arthritis, relapsing polychondritis, amyloidosis, and Kimura disease can also present with epiglottic masses. Focal amyloidosis, more common in the larynx than other head and neck sites, may present as a non-enhancing soft tissue mass with stippled calcification in the epiglottis, showing isointensity on T1- and slight hyperintensity on T2-weighted MRI. Kimura disease, a rare inflammatory condition, can manifest as a polypoid epiglottic mass.
Conclusion
Epiglottic masses encompass a broad differential diagnosis meaning, ranging from benign lesions like squamous papillomas and cysts to malignant tumors, granulomatous diseases, and manifestations of systemic conditions. While otolaryngologists are more likely to clinically identify these masses, radiologists play a crucial role when epiglottic masses are encountered incidentally or require further characterization. Radiologists must be aware of this broad differential and utilize imaging characteristics to narrow the possibilities, thereby contributing significantly to accurate diagnosis and appropriate clinical management, whether the masses are asymptomatic incidental findings or present with airway obstruction.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
References
References from original article should be listed here. (To be added if needed, as per original article)