Pulmonary tuberculosis (TB) commonly manifests as cavitary lesions and infiltrates, typically in the upper lobes of the lungs. Lower lobe involvement and atypical radiological presentations, such as masses or solitary nodules, are less frequent. However, in immunocompromised individuals, these atypical presentations, including the extremely rare “cannon ball” appearance, are increasingly observed. The differential diagnosis for cannon ball lesions in the lung is broad, encompassing metastasis, fungal infections, and granulomatous diseases like Wegener’s granulomatosis and sarcoidosis. This case report highlights a middle-aged woman with diabetes mellitus who presented with unusual symptoms and multiple lung nodules resembling cannon balls on imaging, ultimately diagnosed as pulmonary tuberculosis. This case underscores the importance of considering TB in the differential diagnosis of cannon ball lung lesions, particularly in immunocompromised patients and TB-endemic regions.
Case Presentation
A 43-year-old woman, a non-smoking homemaker with a vegetarian diet, was admitted with a two-month history of dry cough, accompanied by abdominal pain, low-grade fever, decreased appetite, and unintentional weight loss over the preceding 15-20 days. She denied chest pain, hemoptysis, dyspnea, nausea, vomiting, or urinary symptoms. Her medical history included well-controlled diabetes mellitus for two years, managed with oral hypoglycemic agents. She reported no occupational exposures, addiction history, or biomass fuel exposure.
Physical examination revealed normal vital signs, except for a slightly elevated pulse rate of 90 bpm and a respiratory rate of 20 bpm. Blood pressure was 110/70 mmHg. Systemic examination was unremarkable, with no pallor, clubbing, cyanosis, jaundice, lymphadenopathy, or edema. Respiratory auscultation revealed bilaterally equal breath sounds with fine crepitations in all lung fields. Abdominal examination was normal, without organomegaly, distension, tenderness, guarding, or rigidity. Cardiovascular, urogenital, and breast examinations were also normal.
Initial laboratory investigations showed a hemoglobin level of 13 g/dL and a white blood cell count of 8700/mm3 (56% polymorphonuclear cells, 40% lymphocytes). The erythrocyte sedimentation rate (ESR) was significantly elevated at 120 mm/h. Urine analysis, stool examination, and biochemical profiles (renal and liver function) were within normal limits. Tumor markers (CEA 19-9, CA-125) were also within normal ranges. Sputum microscopy for acid-fast bacilli (AFB) and Gram stain, along with bacterial and fungal cultures, were negative.
Radiological Findings
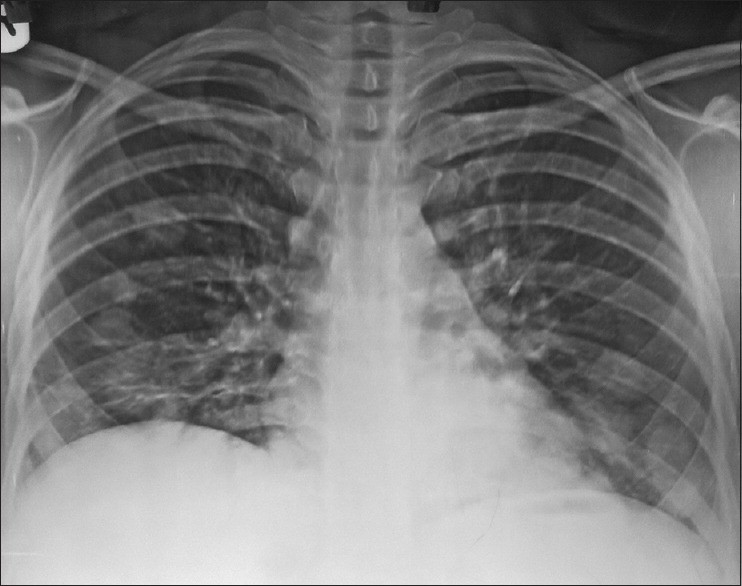
Initial chest radiography (posteroanterior view) revealed multiple rounded opacities bilaterally, predominantly in the lower lung zones, suggesting a nodular pattern.
Figure 1: Chest X-ray demonstrating multiple nodular opacities across both middle and lower lung fields, indicative of cannon ball lesions differential diagnosis.
Abdominal and pelvic ultrasonography showed only fatty liver changes with mild hepatomegaly, without other abnormalities. Subsequently, a computed tomography (CT) scan of the thorax was performed, revealing multiple, variably sized, round to oval, mildly enhancing nodular lesions scattered throughout both lower lobes, with fewer lesions in the right middle lobe. These lesions exhibited a classic “cannon ball appearance”.
Figure 2: Thoracic CT scan showing multiple lung nodules with a cannon ball appearance, predominantly in the lower lobes, crucial for cannon ball lesions differential diagnosis.
Differential Diagnosis of Cannon Ball Lesions
Based on the clinical presentation, laboratory findings, and radiological features, the differential diagnosis for cannon ball lesions in this patient included:
- Malignancy with Metastasis: Given the chronic cough, weight loss, abdominal pain, and the cannon ball appearance on chest imaging, metastatic malignancy was a primary concern.
- Infectious Diseases: Considering the patient’s diabetes and potential immunocompromised state, various infections, particularly tuberculosis, fungal infections, and nocardiosis, were considered.
- Other Conditions: Vasculitis, autoimmune disorders (sarcoidosis, rheumatoid nodules), and less common entities were also included in the differential.
Malignant Metastasis
Metastatic disease is the most common cause of cannon ball lesions in the lungs. Common primary cancers that metastasize to the lungs include breast, colon, prostate, sarcoma, bladder, neuroblastoma, and Wilms’ tumor. Tumors classically associated with cannon ball metastases are renal cell carcinoma and choriocarcinoma, but other primaries like prostate, synovial sarcoma, and endometrial carcinoma can also present similarly. While investigations were conducted to rule out a primary malignancy, the findings were inconclusive.
Infectious Disorders
In immunocompromised patients, infectious etiologies become more prominent in the differential diagnosis of lung lesions.
Pulmonary Tuberculosis
Pulmonary TB, caused by Mycobacterium tuberculosis, remains highly prevalent in many regions. While typical presentations involve upper lobe cavitation, atypical presentations, including lower lobe involvement and multiple nodules resembling cannon ball lesions, are more frequent in immunocompromised individuals, such as those with diabetes. Diabetes mellitus significantly increases the risk of TB infection and active disease progression. Symptoms in diabetic patients with TB may be subtle due to immune suppression, potentially delaying diagnosis. The patient’s chronic cough, low-grade fever, weight loss, elevated ESR, and diabetic status raised suspicion for TB, despite the atypical radiological presentation.
Fungal Infections
- Histoplasmosis: While more common in specific geographic areas, histoplasmosis, caused by Histoplasma capsulatum, can present with pulmonary nodules mimicking metastasis. Immunocompromised individuals are at higher risk for disseminated disease. Epidemiological factors and specific radiographic features like hilar prominence and calcification can aid in diagnosis, but were not prominent in this case.
- Pulmonary Cryptococcosis: Cryptococcus neoformans infection typically affects immunocompromised patients but can occur in healthy individuals. Pulmonary cryptococcosis can range from asymptomatic nodules to severe respiratory distress. Radiological presentations are varied, including multiple nodules, solitary nodules, or masses.
- Nocardiosis: Pulmonary nocardiosis, caused by Nocardia species, is a rare infection primarily affecting immunocompromised individuals. It can mimic TB clinically and radiologically, with variable chest radiographic findings including consolidations, nodules, and masses. Lower lobe involvement and lack of cavitation in this case made nocardiosis less likely.
Parasitic Diseases
- Hydatidosis: Caused by Echinococcus granulosus, hydatid disease can affect the lungs, presenting as cystic lesions or, less commonly, solid nodules. While lung involvement is secondary to liver involvement in most cases, isolated pulmonary hydatidosis is possible. The patient’s lack of animal exposure and normal liver ultrasound made hydatidosis less probable.
Other Conditions
Vasculitis
- Wegener’s Granulomatosis (Granulomatosis with Polyangiitis): This necrotizing vasculitis can involve the lungs, presenting with nodules, masses, and ground-glass opacities. However, typical Wegener’s granulomatosis also involves the upper airways and kidneys, which were not affected in this patient. Negative c-ANCA results further reduced the likelihood of Wegener’s.
Sarcoidosis
Sarcoidosis, a multisystem granulomatous disease, commonly affects the lungs. While hilar lymphadenopathy and interstitial lung disease are typical, macronodular sarcoidosis can rarely present as cannon ball lesions. The lower lobe predominance and absence of hilar lymphadenopathy made sarcoidosis less typical in this case.
Rheumatoid Nodules
Rheumatoid nodules in the lung are rare in rheumatoid arthritis (RA) and are typically associated with long-standing, active RA, and rheumatoid factor positivity. These nodules are often multiple, cavitate, and are located in the upper lung zones. The patient lacked any history or clinical signs of RA.
Pathological Diagnosis and Treatment
Given the inconclusive clinical and radiological findings, a CT-guided lung biopsy was performed. Histopathological examination revealed granulomatous inflammation with central caseous necrosis, Langhans giant cells, and epithelioid cells, consistent with tuberculosis.
Figure 3: Histopathology demonstrating granulomatous inflammation with caseous necrosis, confirming the diagnosis in the cannon ball lesions differential diagnosis.
Based on the histopathology and clinical context, pulmonary tuberculosis was diagnosed. The patient was initiated on a 6-month anti-tuberculosis regimen, including a 2-month intensive phase with rifampicin, isoniazid, pyrazinamide, and ethambutol, followed by a 4-month continuation phase with rifampicin and isoniazid.
Follow-up and Outcome
Following anti-TB treatment, the patient showed significant clinical and radiological improvement. Follow-up chest X-ray and CT scan demonstrated near-complete resolution of the lung nodules.
Figure 4: Follow-up chest X-ray showing resolution of pulmonary opacities after anti-tuberculosis treatment, confirming the diagnosis in the cannon ball lesions differential diagnosis.
Figure 5: Follow-up CT scan confirming clearance of cannon ball opacities after anti-tuberculosis therapy, crucial for cannon ball lesions differential diagnosis and management.
The final diagnosis was bilateral pulmonary nodules due to tuberculosis in a patient with diabetes mellitus.
Discussion and Conclusion
Cannon ball lesions, characterized by multiple, well-defined, rounded lung opacities, most commonly suggest metastatic disease. However, this case highlights pulmonary tuberculosis as a rare but critical differential diagnosis, especially in immunocompromised individuals and TB-endemic regions. While malignancy often tops the differential for cannon ball lesions, other etiologies, including fungal infections, vasculitis, parasitic diseases, and atypical presentations of TB, must be considered.
This case emphasizes that in regions with high TB prevalence, and in patients with risk factors like diabetes, tuberculosis should be high on the differential diagnosis list for cannon ball lung lesions, even when radiological presentations are atypical. Thorough diagnostic workup, including lung biopsy, is essential to differentiate TB from other causes of cannon ball lesions and ensure timely and appropriate management. The successful treatment and resolution of lesions in this case with anti-TB therapy further support the diagnosis and underscore the importance of considering TB in the differential diagnosis of cannon ball appearance, particularly in relevant epidemiological and clinical contexts.
References
[1] ref1 – Original article reference 1
[2] ref2 – Original article reference 2
[3] ref3 – Original article reference 3
[4] ref4 – Original article reference 4
[5] ref5 – Original article reference 5
[6] ref6 – Original article reference 6
[7] ref7 – Original article reference 7
[8] ref8 – Original article reference 8
[9] ref9 – Original article reference 9
[10] ref10 – Original article reference 10
[11] ref11 – Original article reference 11
[12] ref12 – Original article reference 12
[13] ref13 – Original article reference 13
[14] ref14 – Original article reference 14
[15] ref15 – Original article reference 15
[16] ref16 – Original article reference 16
[17] ref17 – Original article reference 17
[18] ref18 – Original article reference 18
[19] ref19 – Original article reference 19
[20] ref20 – Original article reference 20
[21] ref21 – Original article reference 21
[22] ref22 – Original article reference 22
[23] ref23 – Original article reference 23
[24] ref24 – Original article reference 24