Carcinoid heart disease represents a rare yet significant cardiac manifestation of carcinoid tumors, primarily impacting the tricuspid and pulmonary valves. As automotive experts at xentrydiagnosis.store, while our primary focus is vehicle diagnostics and repair, understanding complex medical conditions like carcinoid heart disease, especially its diagnosis, can broaden our knowledge base and highlight the intricate nature of diagnostic processes across different fields. This article delves into the diagnosis of carcinoid heart disease, aiming to provide a comprehensive and SEO-optimized resource for an English-speaking audience.
Aetiology and Pathophysiology
Carcinoid tumors, originating from neuroendocrine cells, are malignant neoplasms with a predilection for the gastrointestinal system. The appendix and terminal ileum are the most common sites. These tumors, when malignant and metastasized, particularly to the liver, can lead to carcinoid syndrome. This syndrome is characterized by a constellation of symptoms including facial flushing, severe secretory diarrhea, and bronchoconstriction. Approximately half of those with carcinoid syndrome go on to develop carcinoid heart disease, predominantly affecting the right side of the heart.
The cardiac complications arise not from direct tumor metastasis to the heart, but from the paraneoplastic effects of vasoactive substances released by the tumor cells. These substances, including serotonin (5-hydroxytryptamine or 5-HT), histamine, tachykinins, and prostaglandins, are normally inactivated by the liver, lungs, and brain. However, when liver metastases are present, these substances bypass hepatic inactivation and reach the heart in significant quantities, particularly affecting the right side due to pulmonary inactivation.
The hallmark pathological finding in carcinoid heart disease is the formation of fibrous endocardial plaques. These plaques can affect the tricuspid valve, pulmonary valve, cardiac chambers, venae cavae, pulmonary artery, and coronary sinus. The fibrous tissue distorts the valves, leading to stenosis, regurgitation, or a combination of both. While right-sided heart involvement is predominant due to pulmonary inactivation of vasoactive substances, left-sided involvement (in 5-10% of cases) suggests extensive liver metastases, bronchial carcinoid, or a patent foramen ovale.
Animal studies and clinical observations, such as those related to the serotonin-releasing appetite suppressant fenfluramine, suggest that serotonin and bradykinin play a direct role in plaque formation and subsequent valvular distortion.
Natural History
Carcinoid tumors are typically slow-growing, and the associated symptoms can persist for many years. However, the onset of cardiac pathology in a patient with a carcinoid tumor signifies a poorer prognosis. Survival rates significantly decrease after the development of carcinoid heart disease. Studies indicate a considerably reduced mean survival time for patients with carcinoid heart disease compared to those without cardiac involvement. Despite this, evidence suggests that addressing the cardiac complications of carcinoid heart disease through treatment can improve both symptoms and longevity.
Clinical Presentation
Diagnosing carcinoid heart disease requires a high degree of clinical suspicion. Carcinoid syndrome symptoms usually manifest between the fifth and seventh decades of life. The latency between the onset of carcinoid symptoms and the diagnosis of carcinoid heart disease can range from two to five years. The classic carcinoid syndrome symptoms—flushing, diarrhea, and bronchospasm—should raise suspicion for potential cardiac involvement, as approximately 50% of patients with these symptoms develop carcinoid heart disease.
Physical examination may reveal a systolic murmur along the left sternal border, indicative of tricuspid regurgitation, a common finding. Murmurs associated with pulmonary stenosis or regurgitation might also be present. Pellagra, characterized by dermatitis in sun-exposed areas, can also occur due to the tumor’s high nicotinic acid turnover.
The majority of patients with carcinoid heart disease present with signs of right heart failure resulting from severe tricuspid and pulmonary valve dysfunction. Tricuspid valve disease, predominantly regurgitation, is seen in the vast majority of cardiac involvement cases. Pulmonary valve pathology, also frequently regurgitation and sometimes stenosis, is also common. Left-sided involvement, mainly mild to moderate mitral regurgitation, is less frequent.
Unusual presentations, such as pure right heart failure without typical carcinoid syndrome features or constrictive pericarditis mimicking valve dysfunction, have been reported, highlighting the diagnostic challenges. Cardiac metastases from carcinoid tumors are exceedingly rare.
Labile blood pressure, manifesting as either hypotension or hypertension, can be observed in patients with carcinoid heart disease, depending on the circulating levels of different vasoactive substances. Serotonin, for instance, can induce tachycardia and hypertensive crises that are resistant to conventional treatments.
Diagnosis
Routine diagnostic tests like a 12-lead ECG and chest X-ray are of limited diagnostic utility in carcinoid heart disease. ECGs can be normal in a significant percentage of patients, with non-specific ST segment changes and sinus tachycardia being the most common abnormalities. Chest X-rays are also frequently normal or show non-specific findings such as cardiomegaly or minor pulmonary changes.
The cornerstone investigations for diagnosing carcinoid heart disease are:
- 24-hour urinary excretion of 5-hydroxyindole acetic acid (5-HIAA)
- Transthoracic echocardiography
Biochemical Screening
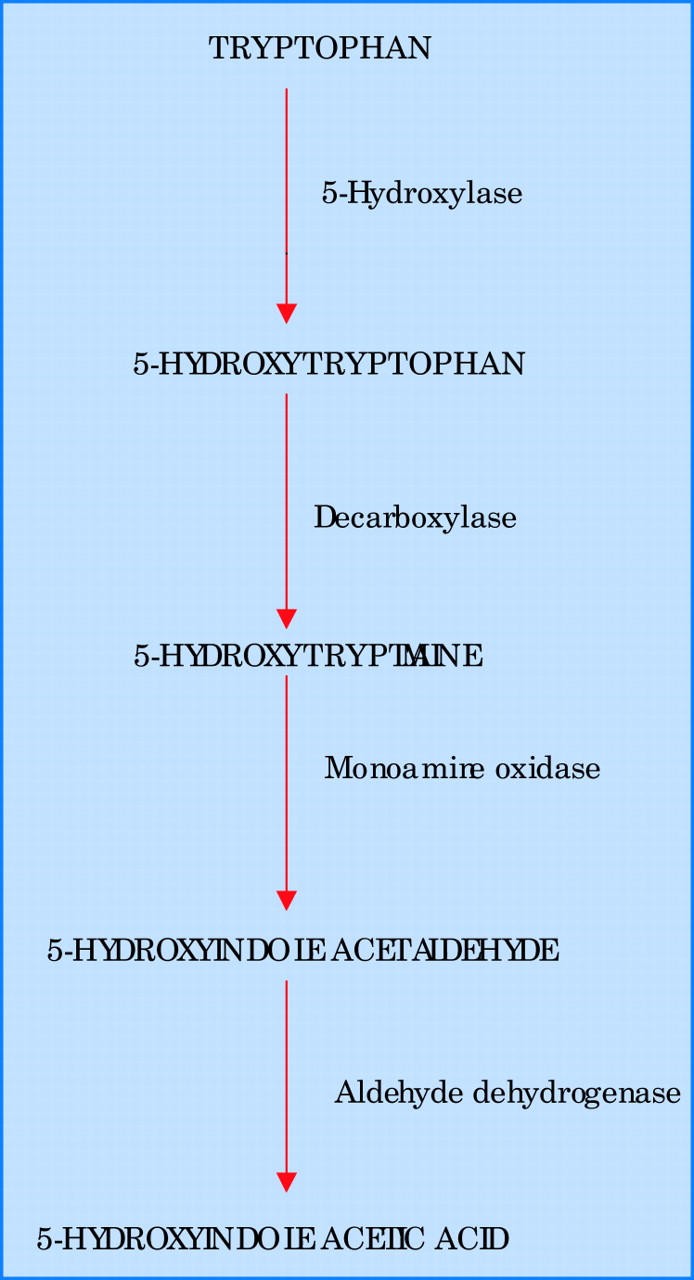
Alt text: Serotonin synthesis and degradation biochemical pathway, illustrating the conversion of tryptophan to 5-HIAA, a key diagnostic marker for carcinoid tumors.
Carcinoid tumors metabolize tryptophan into serotonin, which is then broken down into 5-HIAA. Elevated 24-hour urinary 5-HIAA levels are a hallmark of carcinoid syndrome. In patients with carcinoid heart disease, these levels are significantly elevated, often tenfold higher than normal. This elevation correlates with the severity of cardiac damage, as higher levels of vasoactive substances, particularly serotonin, are thought to contribute to fibroblast proliferation and cardiac plaque formation. Interestingly, 5-HIAA levels may be higher in patients without interatrial shunts, suggesting more active disease.
It’s crucial to note that certain dietary items, such as bananas, nuts, pineapple, kiwi, and avocado, can falsely elevate urinary 5-HIAA levels, leading to false-positive results. Conversely, levodopa, a medication for Parkinson’s disease, can falsely lower 5-HIAA concentrations, potentially leading to false-negative results.
Transthoracic Echocardiography
Echocardiography is pivotal in both diagnosing and assessing the prognosis of carcinoid heart disease. It is the primary imaging modality for evaluating cardiac involvement in patients with carcinoid syndrome. Echocardiographic findings in carcinoid heart disease commonly include right atrial and right ventricular enlargement, and ventricular septal wall motion abnormalities.
Alt text: Echocardiogram showing carcinoid heart disease affecting the tricuspid valve, demonstrating thickened leaflets and severe tricuspid regurgitation with color flow Doppler.
The tricuspid valve leaflets and subvalvar structures often appear thickened, shortened, and retracted, resulting in incomplete valve closure and typically moderate to severe tricuspid regurgitation. Color flow Doppler imaging vividly demonstrates this regurgitation. The continuous-wave Doppler profile of tricuspid regurgitation often displays a characteristic “dagger-shaped” spectrum, with a rapid early peak and decline in pressure.
Alt text: Continuous wave Doppler echocardiography profile illustrating the dagger-shaped spectrum of severe tricuspid regurgitation in carcinoid heart disease, characterized by rapid early peak pressure.
The pulmonary valve may also exhibit thickening and retraction, leading to pulmonary regurgitation and, less frequently, pulmonary stenosis. The combination of severe tricuspid regurgitation and pulmonary stenosis is particularly detrimental, significantly exacerbating right heart failure. Notably, calcification of the affected valves is rare in carcinoid heart disease and its absence can be a helpful negative diagnostic feature.
Treatment
In cases of non-metastatic carcinoid tumors, surgical resection can be curative. However, for patients with carcinoid syndrome, treatment is generally palliative due to the presence of metastases. Surgical tumor debulking and, in cases of liver metastases, hepatic artery ligation or embolization can provide symptomatic relief.
For carcinoid heart disease, management focuses on:
- Heart failure management
- Pharmacotherapy to reduce tumor product secretion
- Surgical/interventional treatment of valvular pathology
Heart Failure Management
General heart failure management strategies, such as salt and water restriction, fluid balance monitoring, and weight management, are crucial. Compression stockings and mobility can help prevent deep vein thrombosis and edema-related skin breakdown. Right heart failure is typically managed with loop diuretics and digoxin. Thiazide diuretics may be added if further diuresis is required. Digoxin is used to improve right ventricular contractility, although data specifically for right-sided heart failure without concomitant lung disease or pulmonary hypertension are limited.
Pharmacotherapy
Somatostatin analogues, like octreotide and lanreotide, have shown to improve symptoms and survival in carcinoid heart disease. Octreotide reduces the secretion of vasoactive peptides by binding to somatostatin receptors, leading to symptomatic relief from diarrhea and flushing, and biochemical improvement reflected in reduced 5-HIAA urinary excretion and serum 5-HT concentrations. Blood pressure and blood glucose monitoring are essential during octreotide administration. Lanreotide offers the advantage of less frequent administration.
Interferon-alpha may also be used to control tumor product secretion and potentially reduce tumor size, sometimes in conjunction with somatostatin analogues. However, neither interferon nor octreotide has been shown to reverse existing cardiac damage from carcinoid disease.
Surgical and Interventional Treatment
Balloon valvuloplasty may offer symptomatic relief for stenotic tricuspid or pulmonary valves, although symptom recurrence is possible. Valve surgery remains the definitive treatment for severe right heart failure in suitable candidates, particularly as severe tricuspid regurgitation is a major cause of mortality in carcinoid heart disease. Early surgical intervention after the onset of cardiac symptoms is generally preferred to avoid worsening right ventricular failure and increased surgical risk. Perioperative octreotide and ketanserin may be used to manage intraoperative hypotension and hypertensive crises, respectively. Antihistamines and corticosteroids are also used preoperatively to prevent flushing, bronchospasm, and reduce bradykinin production.
In tricuspid valve replacement, bioprosthetic valves are often favored over mechanical valves due to the high bleeding risk associated with anticoagulation in patients with liver metastases, despite the potentially shorter lifespan of bioprosthetic valves. Tricuspid valve repair is often not feasible due to valve leaflet restriction. Pulmonary valve replacement may be preferred over valvectomy to reduce postoperative right heart dilatation.
Carcinoid Heart Disease: Key Points for Diagnosis
- Carcinoid Heart Disease Diagnosis hinges on recognizing the cardiac complications arising from neuroendocrine tumors, primarily in the gastrointestinal system.
- Carcinoid syndrome, characterized by flushing, diarrhea, and bronchospasm, is a strong indicator for potential carcinoid heart disease.
- Elevated 24-hour urinary 5-HIAA levels are a key biochemical diagnostic finding.
- Transthoracic echocardiography is the primary imaging modality for diagnosing and assessing the severity of carcinoid heart disease, revealing characteristic valve abnormalities and right heart enlargement.
- Prompt diagnosis and management are crucial for improving patient outcomes and longevity in carcinoid heart disease.
- While treatment focuses on symptom palliation and slowing disease progression, surgical valve intervention can significantly improve quality of life and survival in selected patients.
Successful treatment of carcinoid heart disease, including surgical intervention, has been shown to improve both longevity and quality of life. However, surgical mortality can be higher in older patients and those with significant comorbidities. Preoperative management of carcinoid activity with medication and meticulous perioperative care can improve surgical outcomes.
Acknowledgments
The authors of the original article confirm the content and its originality, stating no conflicts of interest.