Anxiety disorders stand as the most widespread mental health conditions globally. Often overshadowed by conditions like schizophrenia, depression, and bipolar disorder, their impact can be equally debilitating. The diagnostic landscape of anxiety disorders is continually evolving, with both dimensional and structural approaches playing roles in clinical practice and research. These methodologies have been considered for classifications within the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), yet each presents inherent limitations. Contemporary diagnostic emphasis is increasingly leaning towards neuroimaging and genetic research, driven by the need for a deeper understanding of the interplay between biological factors, stress, and genetics in shaping anxiety symptoms.
Effective treatments for anxiety disorders encompass both psychopharmacological interventions and cognitive-behavioral therapies. Given their distinct symptom targets, further research into synergistic combinations of these strategies is crucial for enhancing patient outcomes. The field is also witnessing the emergence of innovative alternative strategies for anxiety management, particularly for treatment-resistant cases. Future advancements should prioritize the development of accessible diagnostic algorithms for primary care settings and place greater emphasis on mitigating functional impairment in individuals living with anxiety.
INTRODUCTION
Anxiety disorders affect a significant portion of the population, with prevalence rates reaching up to 13.3% in the United States, making them the most common category of mental disorders.1 Their extensive presence was initially highlighted in the Epidemiological Catchments Area study over two decades ago.2 Despite this widespread impact, anxiety disorders often do not receive the same level of recognition as other major psychiatric syndromes like mood and psychotic disorders. Furthermore, primary care physicians frequently serve as the initial point of assessment and treatment.3,4 This management context underscores the significant contribution of anxiety disorders to decreased productivity, elevated morbidity and mortality rates, and an increased risk of substance abuse within a substantial segment of the population.5–7
The DSM IV-TR, a previous version of the diagnostic manual, categorized anxiety disorders as outlined in Table 1.8
Table 1.
Anxiety Disorders
| Panic Disorder (PD) |
|---|
| Specifier: with or without Agoraphobia |
| Panic Disorder with Agoraphobia (AG, PDA) |
| Social Phobia (SP) / Social Anxiety Disorder (SAD) |
| Specifier: Generalized |
| Specific Phobias (SPP) |
| Specifier: Animal, Environmental, Blood-Injection-Injury, Situational Type |
| Post-traumatic Stress Disorder (PTSD) |
| Specifier: Acute versus Chronic, with Delayed Onset |
| Acute Stress Disorder |
| Obsessive–Compulsive Disorder (OCD) |
| Specifier: With Poor Insight |
| Anxiety Disorders Due to: |
| Specifier: With Generalized Anxiety, With Panic Attacks, With Obsessive–Compulsive Symptoms |
Advances in anxiety research from the past decade have influenced the diagnostic criteria in the DSM-5,9 published in May 2013. Notably, PTSD and OCD have been reclassified into distinct domains: Trauma and Stressor-Related Disorders, and Obsessive-Compulsive and Related Disorders, respectively.10,11 This reflects a growing understanding of their unique characteristics and underlying mechanisms.
This article will delve into the diagnostic challenges associated with anxiety disorders. It will introduce a model explaining the development and progression of anxiety symptoms, highlight the neurotransmitter systems involved, and evaluate the efficacy of both pharmacological and non-pharmacological treatment approaches currently available.
DIAGNOSTIC DILEMMAS
Over the last decade, epidemiological data has been instrumental in refining the diagnostic boundaries of anxiety disorders. This evolution is evident in the progression from DSM III through IIIR and DSM IV-TR (as seen in Table 1), culminating in DSM-5. However, the high rate of comorbidity among anxiety disorder patients, as revealed by the National Comorbidity Survey (NCS),11 presents a significant challenge to this refinement. Comorbidity is particularly prevalent in Generalized Anxiety Disorder (GAD) and Social Anxiety Disorder (SAD), where it is more often the norm than the exception.12 Clinical practice and research frequently encounter patients exhibiting two or more diagnosable conditions or symptomatic overlap with several sub-syndromal states. This overlap is especially pronounced between different anxiety disorders, depression, and substance use disorders.13
Another complicating factor is the sequential emergence of different disorders within the same individual over time. For instance, a patient might initially present with panic disorder that resolves with treatment, only to later develop symptoms aligning more closely with OCD or GAD. It remains unclear whether this reflects an underlying predisposition or represents distinct, separate conditions.
The current diagnostic framework for anxiety disorders is further challenged by the lack of identified etiological factors and specific treatments for each diagnostic category. Genetic studies utilizing molecular biology techniques have not yet pinpointed single genes or gene clusters as causal factors for specific anxiety disorders, despite some genetic findings related to OCD and panic disorder.14,15 Family and twin studies, however, indicate the significant role of genetic factors, potentially shared across various anxiety disorders, depression, and substance use disorders, even without specific gene identification.16
Despite these diagnostic uncertainties, the effectiveness of serotonergic medications across a range of categorical disorders, including mood and anxiety disorders, has led to suggestions that a dimensional model might be more appropriate for studying and treating these conditions.17 This perspective views a disorder as a complex constellation of co-occurring symptom dimensions, such as panic, social anxiety, and obsessions. Each dimension’s variability could be influenced by biological or genetic factors, potentially requiring distinct treatment approaches.9 The debate between dimensional and categorical approaches remains active in both research and clinical practice, forming a key rationale behind the DSM-5 revisions.18,19
The concept of “spectrum disorders” has emerged within psychiatry, initially for OCD, to address similarities between distinct disorders.20 This concept proved useful in understanding shared responses to pharmacological and psychological treatments and has expanded to encompass spectra like social anxiety, panic-agoraphobia, and post-traumatic disorders.21–23 While helpful, this approach can be overly broad, potentially grouping disorders with limited commonalities, such as pathological gambling and body dysmorphic disorder (BDD) within the OCD spectrum. Neuro-circuitry and genetic investigations have yet to fully validate this spectrum concept.
Dimensional and categorical diagnoses in the DSM-IV-TR typically arise from cross-sectional comparisons of different patient groups. However, clinical presentations unfold within individuals over time, suggesting a need to understand them as part of a psychopathological process. For instance, OCD might be diagnosed based on obsessions or compulsions, but compulsions often develop later as a coping mechanism to manage the anxiety linked to obsessive thoughts.24
This perspective parallels medical disease, where symptoms often represent a combination of a harmful agent and the body’s response. For example, lung scarring in tuberculosis, initially protective, can become detrimental in the long term.
Recognizing the potential commonalities in the processes underlying anxiety and fear across different disorders has spurred the adoption of uniform treatment protocols in primary care25 and the development of unified theories of anxiety.26
THE ‘ABC’ MODEL OF ANXIETY
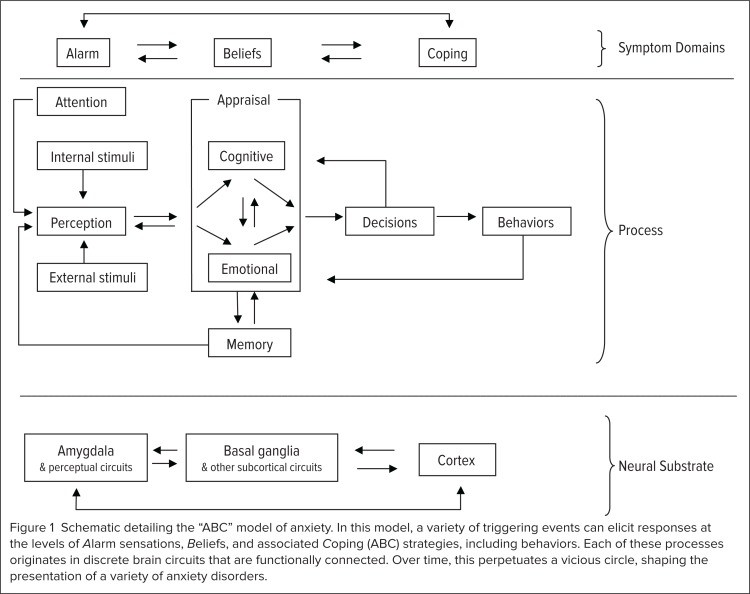
A deeper understanding of the interplay between emotional reactivity, core beliefs, and coping strategies over time is essential for refining diagnoses and improving the management of anxiety disorders. A mathematical model utilizing nonlinear dynamics was recently applied to describe these interactions,27 and subsequently expanded to encompass diagnostic presentations and their underlying processes.28 This model, termed the “ABC model of anxiety,” posits an interaction between alarms, beliefs, and coping strategies (Figure 1).
Figure 1.
Schematic representation of the “ABC” model of anxiety, illustrating the interplay of Alarms, Beliefs, and Coping strategies in shaping anxiety disorders. Triggering events initiate responses at these three levels, originating in functionally connected brain circuits. This interaction creates a perpetuating cycle that defines the presentation of various anxiety disorders over time.
Alarms (A) are defined as emotional sensations or physiological responses to a triggering situation, sensation, or thought. A specific network of brain circuits rapidly processes information related to these alarms.
Beliefs (B) shape the subsequent decision to act, heavily influenced by past experiences, personal and cultural background, and sensory input. Individuals with anxiety disorders often exhibit heightened attention to perceived danger compared to those without anxiety.29 Accurate decision-making regarding beliefs can be hampered by an overwhelming influx of details, leading to catastrophic thinking and indecisiveness.
This, in turn, dictates coping strategies (C), which are behaviors or mental activities aimed at reducing anxiety and evading perceived danger. Coping strategies are deemed adaptive or maladaptive based on their effectiveness in alleviating anxiety. The interplay of these processes over time forges the complex picture of a specific anxiety disorder.
Panic disorder, for instance, might begin with an initial panic attack driven by the brain’s alarm networks. This event activates circuits processing danger information, and coupled with individual beliefs about the event, heightens concerns about health and safety. This then leads to coping mechanisms aimed at reducing perceived danger, such as medical evaluations that may temporarily alleviate fear.
While these processes are common in healthy individuals facing unpleasant situations, in panic disorder, medical reassurance often proves insufficient due to the need for absolute certainty of “no danger.” This unattainable assurance perpetuates worry and anticipation of future attacks. Consequently, patients increase safety-seeking behaviors, such as repeated medical exams and reliance on a “safe” person.
Unfortunately, because absolute safety is elusive, these behaviors become more entrenched and chronic in an attempt to manage anxiety. The persistence of anxiety further fuels worry and distress, perpetuating a cycle of recurrent panic attacks. Uninterrupted, this pattern can escalate into maladaptive coping behaviors like agoraphobia and comorbid depression. This process is broadly applicable across anxiety disorders, though specific stages may dominate in different conditions; for example, ritualistic behavior is prominent in OCD, while avoidance is characteristic of social anxiety disorder.
Clinical experience indicates that patients readily grasp and interpret their symptom patterns within the ABC model. This model is effectively integrated with medication and behavioral techniques in treatment, as demonstrated in prior research.30 The ABC model is also a valuable tool for teaching psychiatric residents, facilitating their understanding and application of cognitive-behavioral therapy (CBT) within a relatively short timeframe.
Interplay Between Biological and Psychological Factors
Effective treatment of anxiety disorders necessitates understanding their development and the factors that sustain them. Recent years have yielded greater insights into the interaction of genetic, biological, and stress factors shaping the presentation of these disorders, although the precise inherited factors remain unclear.
One hypothesis suggests that abnormal cognition could be an inherited vulnerability. Cognitive theory emphasizes the central role of abnormal or “catastrophic” cognition as a fundamental mechanism underlying all anxiety disorders. Most cognitive treatment and research strategies were developed based on this premise.
The ABC model underscores the interaction between information processing and emotional and cognitive processes, which are governed by overlapping brain circuits competing for the same neural resources.27
In many anxiety disorders, patients process fear-inducing information with excessive detail, overwhelming their capacity for proper appraisal. They often resort to binary categorization of information into “good” or “bad,” lacking nuance. This leads to worst-case scenario thinking (catastrophizing) and defensive actions against perceived threats.
Stress
Stress is a significant contributor to the pathology of anxiety disorders. PTSD, for example, is defined by stress as the primary etiological factor, although high levels of co-occurring stress are also reported in other anxiety disorders. While the role of stress may be less obvious in GAD and OCD, patients frequently link the onset of their disorder to a significant stressful event or chronic stressor. Increased stress reactivity, whether a cause or a consequence, can trigger relapses in chronic anxiety conditions like GAD. Research suggests that stressful events or persistent disorders can induce secondary biological changes in specific brain structures.31,32
The DSM-IV-TR system’s approach to stressors is limited. While stressors are identified separately on Axis IV, the broader context for the patient remains unclear. A more informative approach might involve specifying the source and persistence (immediate, intermittent, constant) and severity (mild, moderate, severe, catastrophic) of stress. This would allow for a more comprehensive understanding of the stress landscape and its dynamics. For example, panic disorder stemming from combat trauma may differ clinically from panic disorder triggered by chronic work stress or family separation. Further research is needed to explore the impact of stress on the biology and course of anxiety disorders.
Biological Factors
Biological factors are of paramount importance in understanding anxiety disorders. Anxiety disorders can manifest in the context of medical illnesses,33 highlighting a complex interplay between physical and mental health. This relationship can be multifaceted:
First, metabolic or autonomic abnormalities resulting from medical illness can directly induce anxiety symptoms (e.g., hyperthyroidism causing panic attacks). Medical symptoms can also trigger anxiety (e.g., heart arrhythmia sensations triggering panic). In some cases, medical conditions can mimic anxiety disorders (e.g., perseverations in intellectual disability mistaken for OCD). Finally, medical illness and anxiety disorders can simply coexist independently. An intriguing interaction involves Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections (PANDAS), linked to a subset of OCD cases.34
Over the past two decades, biological research on anxiety disorders has shifted focus from peripheral measures of autonomic and neurochemical parameters to direct investigation of brain reactivity and neurochemistry using neuroimaging. Anxiety disorders are well-suited for neuroimaging research due to the ease of provoking specific symptoms in many cases. Research into neural circuits has largely drawn on models of anxiety and fear developed by basic scientists,35,[36](#b36-ptj3801030] with syntheses of current data attempted for panic disorder37 and OCD.38
While comprehensive reviews of neuroimaging studies in anxiety exist,39,40 the picture remains incomplete, partly due to a lack of clinical trials examining the long-term integration of threat responses. Consistent with the dynamical model, each anxiety disorder can be viewed as an interaction of anxious feelings, abnormal information processing, and inadequate coping strategies. Overlapping neuronal circuits are implicated in alarm reactions, threat processing, and behavioral coping (Figure 1). This model simplifies the complex brain circuitry that requires decades of further research to fully understand the brain’s threat processing over time.
For simplicity, we can identify Alarm circuits (A), with the amygdala as a key structure. These circuits also include the periaqueductal gray matter and various brainstem nuclei.41 Disruptions in these circuits can lower the threshold for alarm reactions, leading to spontaneous panic attacks. These circuits are likely responsible for rapid threat responses.
Belief circuits (B), involved in processing “threat” information, are likely closely linked to the basal ganglia, cingulum, and corticostriatal connections, often affected in OCD.
Coping circuits (C) are likely governed by distributed cortical networks and are more difficult to isolate. A helpful mnemonic for these circuits is A (Alarm, amygdala), B (Beliefs, basal ganglia), and C (Coping, cortex).
How Anxiety Affects Neurotransmitters
Neuronal circuits are regulated by multiple neurotransmitter systems, most notably gamma-aminobutyric acid (GABA) and glutamate. The major neurotransmitter systems—serotonin, dopamine, and norepinephrine—have been extensively studied in both normal and pathological anxiety states.40,42 Their significance in anxiety is evident in the fact that most effective treatments target one or more of these systems. However, anxiety disorders are not simply caused by deficiencies in single neurotransmitters. These neurotransmitter networks have intricate interconnections, feedback loops, and complex receptor structures.43 This complexity contributes to unpredictable and sometimes paradoxical medication responses.
Research into other neurotransmitter systems has advanced our understanding of their roles in anxiety but has not yet yielded new treatments. The primary neurotransmitter and receptor systems implicated in anxiety disorder pathogenesis are discussed below.
Serotonin
Serotonergic pathways originate in the raphe nuclei and project widely throughout the forebrain.44 These circuits are crucial for regulating brain states, including anxiety, and modulate dopaminergic and noradrenergic pathways.45 Increased serotonergic tone appears correlated with reduced anxiety, though the underlying mechanism remains unclear.
Numerous serotonin receptor subtypes exist, with varying roles depending on location. For example, the serotonin-1a receptor can both mediate and inhibit serotonergic neurotransmission, depending on whether it is presynaptic or postsynaptic.46 Not all serotonin receptor subtypes mediate anxiolytic effects; serotonin-2a receptor agonism, for instance, underlies the psychedelic effects of LSD and mescaline.47
Despite this complexity, serotonin reuptake inhibitors, which presumably enhance serotonergic neurotransmission, are recognized to reduce anxiety symptoms in many patients.48
Gamma-aminobutyric Acid (GABA)
GABA is the primary inhibitory neurotransmitter in the central nervous system (CNS). Increased GABA neurotransmission mediates the anxiolytic effects of barbiturates and benzodiazepines.49 These medications do not directly bind to GABA receptors but rather promote the open configuration of associated chloride channels. Barbiturates prolong channel opening duration, while benzodiazepines increase opening frequency.
While GABAergic pathway modulation can provide rapid anxiety relief, compensatory mechanisms and the use of barbiturates and benzodiazepines can lead to tolerance and potentially fatal withdrawal.50 Furthermore, these drugs can impair memory encoding, potentially hindering the effectiveness of concurrent psychotherapy.
Anticonvulsant agents, also affecting GABA transmission, are used to treat anxiety.51 This medication class indirectly affects GABA transmission by blocking calcium channels, potentially reducing withdrawal and addiction risks.52
Dopamine
Dopaminergic pathways originate in the midbrain’s ventral tegmental area and substantia nigra, projecting to the cortex, striatum, limbic nuclei, and infundibulum. Dopamine’s role in normal and pathological anxiety is complex and multifaceted.53 Dopamine D2 receptor blockade, characteristic of antipsychotic medications, is also anxiolytic.54
Antipsychotics have been used to treat anxiety. However, dopamine, a catecholamine, is upregulated alongside norepinephrine in anxiety states, while increased dopaminergic signaling can also promote self-efficacy and confidence, potentially reducing anxiety.55, 56 This complexity results in variable responses to dopamine-enhancing medications. Some anxiety disorder patients respond well to pro-dopaminergic drugs like bupropion, while others experience symptom exacerbation.
Norepinephrine
Noradrenergic neurons originate primarily in the locus coeruleus in the pons and project widely throughout the CNS.57 Like dopamine, norepinephrine is a catecholamine upregulated in anxiety states, but its role in anxiety is complex and potentially bidirectional. Many physiological anxiety symptoms are mediated by norepinephrine, and antagonists of various norepinephrine receptor subtypes are used to manage specific anxiety aspects.
For example, propranolol, a beta2-norepinephrine receptor antagonist, reduces rapid heart rate, tremor, and voice quivering associated with performance anxiety.58 While effective for these physiological symptoms of normal anxiety, propranolol is less effective for emotional or cognitive anxiety components and is not typically used for anxiety disorders.
Similarly, prazosin, an alpha1-norepinephrine receptor antagonist, reduces nightmares associated with PTSD but is not effective for other anxiety disorder symptoms.59,60 Serotonin-norepinephrine reuptake inhibitors (SNRIs), like venlafaxine and duloxetine, are effective in treating anxiety disorders.61 These medications also alleviate neuropathic pain and may target the agonal component of anxiety.
Glutamate
Glutamate is the primary excitatory neurotransmitter in the CNS, involved in virtually all neuronal pathways, including those underlying normal and pathological anxiety.62,63 The N-methyl-d-aspartate (NMDA) receptor subtype may be particularly relevant to anxiety disorders, mediating learning and memory. NMDA receptor activation triggers protein synthesis, strengthening neuronal connections when they fire simultaneously. Glutamatergic pathways are likely involved in both conditioning and extinction, processes central to the development and treatment of anxiety disorders.64
Preliminary evidence suggests that both NMDA pathway augmentation and antagonism can be effective in treating anxiety disorders, although no glutamatergic medications are FDA-approved for this purpose. d-cycloserine, enhancing glutamatergic neurotransmission, can augment exposure therapy for anxiety disorders.65 Conversely, NMDA receptor antagonists memantine and riluzole have shown efficacy in OCD treatment.66 Interestingly, memantine appears less effective for GAD, suggesting distinct pathways may underlie different anxiety disorders.67
Other Neurotransmitters
Numerous other neurotransmitter systems contribute to the biological mechanisms of fear and anxiety. Neuropeptides, including substances P, N, and Y; corticotropin-releasing factor (CRF); cannabinoids; and others, modulate fear in animal models.68–70 However, experimental agents targeting these systems have not yet translated into FDA-approved treatments.71 Stringent approval criteria and high placebo responses in anxiety trials may contribute to this lack of translation.72
PHARMACOLOGICAL THERAPY
While numerous neurotransmitters play a role in anxiety, relatively few medication classes are clinically used for anxiety treatment. These classes are briefly discussed below.
Selective Serotonin Reuptake Inhibitors (SSRIs)
SSRIs, typically indicated for depression, are considered first-line therapy for anxiety disorders. This class includes fluoxetine, sertraline, citalopram, escitalopram, fluvoxamine, paroxetine, and vilazodone.72 SSRIs inhibit the serotonin transporter, leading to desensitization of postsynaptic serotonin receptors, normalizing serotonergic pathway activity.
The precise mechanism by which this alleviates anxiety symptoms is not fully understood. Vilazodone, a newer SSRI approved for major depressive disorder, also acts as a partial agonist at the serotonin-1a receptor, potentially contributing to its anxiolytic effects.73 Buspirone, not an SRI but a 5-HT1a agonist, is also frequently used alone or to augment SSRI therapy.74
Serotonin–Norepinephrine Reuptake Inhibitors (SNRIs)
SNRIs, inhibiting both serotonin and norepinephrine transporters, include venlafaxine, desvenlafaxine, and duloxetine.75 Milnacipran is rarely used for anxiety, primarily indicated for fibromyalgia.76 SNRIs are typically used after SSRI failure or inadequate response, or instead of augmenting SSRIs due to the risk of serotonin syndrome from combining these classes.
Patient responses to SNRIs vary; some may experience exacerbated physiological anxiety symptoms due to increased norepinephrine signaling. For others, the increased noradrenergic tone may contribute to anxiolytic efficacy.
Benzodiazepines
While historically prevalent in anxiety treatment, benzodiazepines are no longer considered first-line due to risks associated with chronic use.75 They are highly effective for acute anxiety but carry risks with long-term, high-dose use, including:
- Physiological and psychological dependence.
- Potential for fatal withdrawal.
- Impaired cognition and coordination.
- Risk of lethal overdose when combined with alcohol or opioids.
- Inhibition of memory encoding, interfering with psychotherapy efficacy.
Benzodiazepine use is often restricted to short-term acute anxiety management or as therapy for refractory anxiety after other drug failures. Some patient subgroups do well with low-dose benzodiazepines and can safely taper off, particularly with concurrent cognitive-behavioral therapy (CBT).77
Antiseizure Medications
Due to benzodiazepine side effects, antiseizure agents are increasingly used for anxiety. Initially used as mood stabilizers, their anxiolytic properties were quickly recognized. Gabapentin and pregabalin are commonly used off-label for anxiety.51,78 Less data exists for topiramate, lamotrigine, and valproate.79 In higher doses, antiseizure medications can produce benzodiazepine-like side effects.80
Tricyclic Antidepressants (TCAs)
TCAs function as norepinephrine reuptake inhibitors, and some also inhibit serotonin reuptake. While comparable in efficacy to SSRIs or SNRIs for anxiety, TCAs carry more side effects and are potentially lethal in overdose. Thus, TCAs are rarely used for anxiety, except for clomipramine, which may be more effective than SSRIs or SNRIs for OCD.81
Additional Medications
Hydroxyzine, mirtazapine, nefazodone, and atypical antipsychotics are also used to treat anxiety.82 While effective, particularly for OCD, they are not first-line treatments and are typically adjuncts to SSRIs or SNRIs. Hydroxyzine, indicated for anxiety, likely exerts anxiolysis via histamine H1 and serotonin-2a receptor inhibition.83
TREATMENT STRATEGIES
Initial Treatment Algorithms
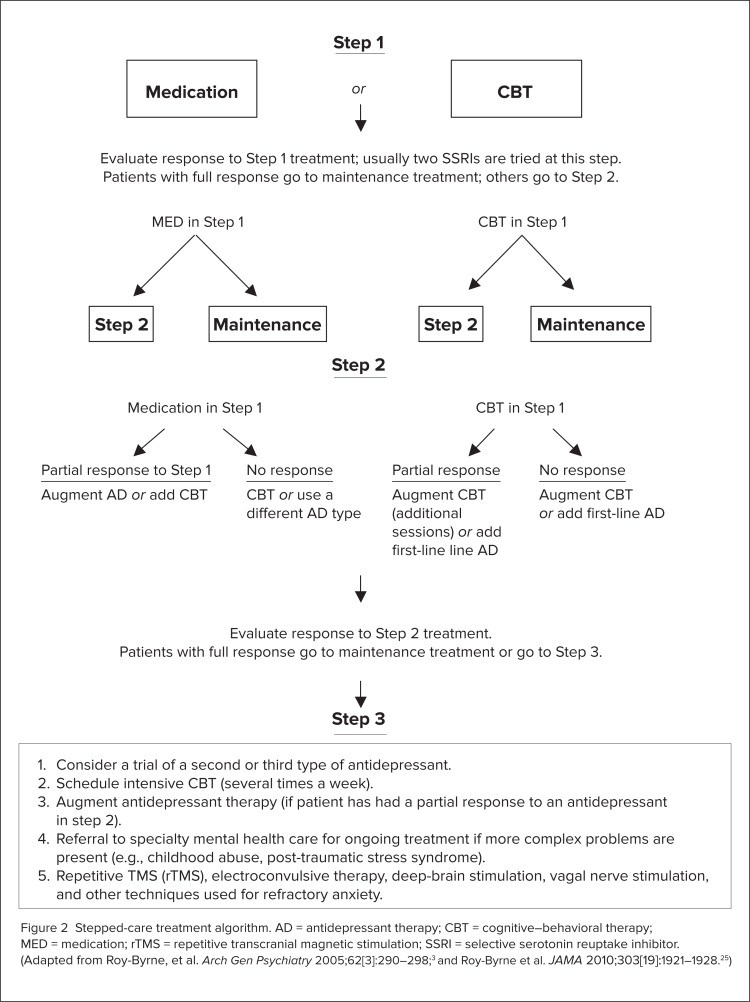
In the 1990s, mainstream psychological and pharmacological anxiety disorder treatments were developed and tested, leading to a similar initial algorithm for major anxiety disorders.84,85 A typical algorithm, adapted from Roy-Byrne et al.,25 is shown in Figure 2.
Figure 2.
Stepped-care treatment algorithm for anxiety disorders, outlining a progression from initial interventions to more intensive treatments. AD = antidepressant therapy; CBT = cognitive–behavioral therapy; MED = medication; rTMS = repetitive transcranial magnetic stimulation; SSRI = selective serotonin reuptake inhibitor. (Adapted from Roy-Byrne, et al. Arch Gen Psychiatry 2005;62[3]:290–298;3 and Roy-Byrne et al. JAMA 2010;303[19]:1921–1928.25)
Generally, clinicians choose between CBT and an SSRI, trying another SSRI if the first is ineffective or poorly tolerated. No SSRI has demonstrated superiority over others. SSRI choice is typically guided by side effect profiles, pharmacokinetic and pharmacodynamic properties, and potential drug interactions.
Several reviews of SSRI therapies for anxiety disorders exist.86 A general SSRI principle is “start low and go slow,” initiating treatment at approximately half the depression dose and gradually titrating upwards, with dosage changes no more frequent than weekly.
Antidepressants with broader mechanisms (e.g., venlafaxine and clomipramine) are considered for non-responders, based on their multi-neurotransmitter effects and limited meta-analytic data supporting their superiority in depression and OCD.87 Benzodiazepines are generally avoided except in acute states or treatment-resistant chronic conditions.
Limited data exists on post-initial treatment steps, such as maintenance therapy duration. Clinical experience suggests treatment continuation until marked symptom reduction is sustained for at least 6 months. More research is needed in this area.
Further research has explored combined treatments at initial and later stages.88,89 In later stages of anxiety treatment, GABAergic antiepileptic drugs and atypical antipsychotics may be considered. Atypical antipsychotics have shown promising efficacy in placebo-controlled anxiety disorder trials.90
Side Effect Profiles
Patients and physicians must be aware of adverse drug reactions. Valuck provides an extensive review of SSRI side effects.91 Studies have linked SSRIs and SNRIs to increased suicidality92 and atypical antipsychotics to tardive dyskinesia and arrhythmias.93 All these drugs can cause weight gain and sexual dysfunction. Polypharmacy, increasingly common especially in complex and treatment-resistant anxiety, necessitates awareness of potential drug-drug interactions.94
Serotonin syndrome and neuroleptic malignant syndrome, while rare, should be considered. SSRI discontinuation withdrawal syndrome, characterized by paresthesias, dizziness, nausea, diaphoresis, and rebound anxiety, is common upon abrupt cessation.95 SSRI and SNRI discontinuation should involve gradual tapering, ideally alongside CBT.
Cognitive–Behavioral Therapy (CBT) and Medications
CBT has strong empirical support for psychological anxiety disorder treatment.96 Treatment algorithms often place CBT alongside SSRIs as a first-line choice (Figure 2). Combination therapy with drugs and CBT has shown varied results compared to monotherapy, depending on the anxiety disorder type.
Meta-analyses comparing combination treatment to monotherapy or CBT suggest CBT may be more successful than medication for anxiety, while medication may hold an advantage for depression.97 Within anxiety disorders, responsiveness to CBT or medication varies, with CBT showing an advantage for panic disorder, and medication potentially more effective for social anxiety disorder.
Choosing between medication or CBT, alone or combined, depends on factors such as therapist availability, CBT affordability (more expensive than medication, especially in primary care), and patient preference.
Cognitive–Behavior Therapy (CBT) Alone
Suboptimal anxiety disorder treatment is often attributed to limited CBT therapists and affordable sessions. Distilling effective therapy principles for primary care settings, emphasizing education and staff training, is crucial.25 Oxford University Press offers excellent therapist and patient manuals.98 The rise of internet-based, self-administered therapies warrants further research into their efficacy.99 Complex anxiety disorders may not be adequately self-treated, while specific phobias might be manageable alone or with support.
Koszycki et al.100 explored self-administered CBT effectiveness alone or optimized by therapist-directed CBT, self-administered CBT, or medication augmented with self-administered CBT. Their findings suggest self-administered treatment can be a valuable addition to the CBT toolkit.
While many anxiety treatments are effective, not all help everyone, and efficacy varies across anxiety disorders. Simple phobias are easier to treat than complex PTSD. SSRIs and CBT are the most empirically supported treatments. CBT relapse rates compared to medication are understudied, but clinical experience suggests CBT offers longer-lasting effects if patients maintain learned skills.
Technique
CBT shares common ground with psychodynamic psychotherapy. Patients seek expert help in a supportive relationship to improve functioning and well-being in a reality-oriented context. However, CBT is directive and collaborative; therapists establish clear goals and use evidence-based techniques to elicit patient’s feelings (Alarm), dysfunctional thoughts (Beliefs), and behaviors (Coping).
The therapeutic relationship is less emphasized as a curative factor in CBT but is vital for building trust and support, enabling patients to examine maladaptive beliefs and behaviors. Therapists explicitly conceptualize the patient’s disorder regarding its genesis, evolution, and maintenance. Manuals and psychoeducational materials are often incorporated, and homework may be assigned to foster adaptive anxiety management, belief change, and coping mechanisms, often through exposure exercises. Patients are often taught the ABC model to understand the dynamic interplay of feelings, thoughts, and behaviors.
Patient compliance directly correlates with treatment effectiveness. Motivational interviewing, exploring the cost-benefit ratio of maladaptive thoughts and behaviors, enhances compliance and effectiveness.101 Patients learn self-monitoring and symptom-reduction techniques to increase motivation to confront anxiety. Breathing and relaxation techniques can be taught as mental hygiene to raise alarm reactivity thresholds and improve awareness of escalating alarm reactions.
Patient thoughts are central to the CBT model of anxiety.102 Belief modification is crucial for alarm downregulation and adaptive coping replacement. While beliefs are key, exposure to anxiety-provoking stimuli is often essential for belief change. Cognitive restructuring techniques aim to reduce catastrophic thinking, facilitating willingness to test beliefs through exposure exercises.
Exposure
Exposure involves gradual and systematic presentation of anxiety-inducing stimuli for sufficient duration to demonstrate that anxiety can decrease without avoidance or escape. For example, dog phobia treatment might progress from picture exposure to standing near a pet shop to holding a dog. Each step is repeated until anxiety diminishes before advancing. This process reduces alarm and modifies the exaggerated belief that all dogs are dangerous to a more accurate view that most pet dogs are not threatening, ideally eliminating phobic avoidance.
Mindfulness (The Third Wave)
Mindfulness-based approaches represent a “third wave” in CBT, following behavioral and cognitive approaches.103 Mindfulness, derived from Buddhist psychology, is defined as “awareness of present experience with acceptance.”103 These therapies are rooted in Jon Kabat-Zinn’s Mindfulness-Based Stress Reduction (MBSR) program from 1979.104
Mindfulness-based cognitive therapy (MBCT) integrates mindfulness into CBT.105 MBCT has been applied to panic disorder and other anxiety disorders, but further controlled research is needed.106 MBCT emphasizes relapse prevention through mindful awareness, helping patients recognize that current symptoms do not necessarily signal relapse.
Acceptance and commitment therapy (ACT) incorporates mindful focus, using meta-cognitive exercises to help patients perceive thoughts and anxiety as separate from their self-concept. Anxiety-provoking thoughts are to be observed and accepted, rather than resisted and changed, contrasting with traditional CBT and Western psychology.107
Shifting Treatment to Primary Care
Anxiety treatment increasingly occurs in primary care due to managed care. Limited primary care physician time contributes to underrecognition and undertreatment of anxiety disorders. Simultaneously, SSRI (antidepressant) use is rising in primary care, with physicians being the largest prescriber group. This presents challenges:
- SSRIs are often prescribed quickly for emotional distress that may not meet anxiety disorder criteria.
- Therapy dosage and duration may be inadequate.
- Adverse effects may be managed only by treatment discontinuation.
This situation may explain why psychiatrists see more patients disillusioned with failed pharmacotherapy attempts.
Another primary care issue is limited behavioral strategy understanding, resulting in low mental health professional referral rates. There is a trend toward developing comprehensive panic disorder treatments for primary care physicians.
One study tested a panic disorder treatment algorithm in primary care.108 This reflects a shift towards psychiatrists becoming consultants to primary care physicians, assisting with initial management and managing severe, treatment-resistant anxiety.
Management of Treatment-Resistant Anxiety
Managing refractory anxiety necessitates re-evaluation of diagnosis, comorbidities, and cognitive, stress-related, and biological factor interplay. Patient and family coping strategies should be reviewed, along with initial treatment doses and durations.
Intensive CBT, combined with adequate SSRI, SNRI, or combination trials, may be needed initially. Treatment can progress to SSRI combinations with antiepileptic or atypical antipsychotics, especially if bipolar or psychotic disorder is suspected.109,110 Partial hospitalization in specialized centers with extensive CBT and medication management may be considered later.111
While other therapies lack demonstrated anxiety disorder efficacy, they may address personality issues in chronically anxious patients.
Experimental and Off-Label Nonpharmacological Treatments
Anxiety disorder therapies beyond conventional treatments, off-label agents, and intensive CBT are largely experimental. Promising medications have included intravenous clomipramine, citalopram, and morphine.109 Many other neurotransmitter-targeted treatments have failed.72
Invasive therapies are emerging for treatment-resistant cases with significant functional impairment, typically severe OCD, targeting brain circuits involved in fear and anxiety processing.
Electroconvulsive Therapy (ECT)
ECT involves brief electrical impulses to the scalp inducing cortical neuronal discharges and seizure activity. While effective for treatment-resistant mood disorders, limited data exists on its anxiety disorder efficacy.112 ECT mechanisms and focal targets are undetermined.
Vagal Nerve Stimulation (VNS)
Initially for epilepsy, VNS was used in psychiatry after mood improvements were observed.113 VNS is thought to stimulate brain networks (amygdala, hippocampus, insula, orbitofrontal cortex) via the vagal nerve, relevant to anxiety and fear processing. VNS is not routinely used for anxiety, and evidence for resistant anxiety disorders is limited.114 No randomized controlled trials have further investigated this intervention.
Repetitive Transcranial Magnetic Stimulation (rTMS)
rTMS uses focal magnetic scalp stimulation to excite or inhibit cortical neurons. Less invasive than ECT, rTMS does not require anesthesia or induce generalized seizures. It can target brain regions implicated in anxiety disorders.
rTMS limitations include inability to reach deeper brain structures involved in OCD (caudate nucleus, thalamus, anterior capsule) or panic disorder (amygdala, hippocampus, anterior cingulate), and lack of stimulation site specificity.
rTMS is not approved for anxiety disorders, likely due to limited large-scale studies. Limited evidence suggests efficacy for OCD, with larger effects reported by altering stimulation sites.115,116 rTMS has shown anxiety symptom improvement in PTSD and panic disorder, but is not yet clinical practice.117
A small GAD study reported anxiety reduction using symptom-provocation fMRI to guide rTMS site selection.118 No rTMS studies exist for social anxiety disorder.
Surgery
Psychosurgery for treatment-resistant anxiety disorders (GAD, panic disorder, social phobia) has shown adverse cognitive outcomes (apathy, frontal lobe dysfunction) in long-term follow-up.119 Surgical approaches are typically reserved for OCD due to significant functional deficits in refractory cases.
Surgical approaches include anterior capsulotomy, anterior cingulotomy, subcaudate tractotomy, and limbic leucotomy.120,121 Cingulotomy is the most common psychosurgical procedure in North America due to efficacy and low morbidity/mortality. Postoperative effects include transient headache, nausea, or urinary difficulty. Postoperative seizures, the most serious side effect, occur in 1-9% of cases.
Patient outcomes are assessed 6 months to 2 years post-procedure, suggesting postoperative neural reorganization is important. Direct lesion approach comparisons are rare. Long-term outcomes show significant therapeutic effects for each procedure, with response rates ranging from 30-70% in remission, response, and functional improvement.
Deep-Brain Stimulation (DBS)
DBS involves implanting electrodes under stereotactic MRI guidance, offering adjustable neurostimulation.122 Electrode stimulation parameters can be modified post-implantation.
Studies with blinded stimulation show moderate results.123 More recently, structures adjacent to the internal capsule have been targeted.124,125 Response rates are consistently around 50%.125
Postoperative complications (infections, lead malfunctions) are more common with DBS due to its prosthetic nature. Batteries require periodic replacement. Stimulation-related side effects include mood, sensory, and cognitive changes, typically stimulation-dependent and reversible with parameter adjustments.
Complementary and Alternative Medicine (CAM)
The 1990s saw the rise of alternative anxiety treatment strategies,126 including herbal medications (St. John’s wort), vitamins, supplements, magnetic and EEG synchronizing devices, “energy” treatments, and meditation-based therapies.
CAM treatments may be provided within healthcare models like acupuncture, homeopathy, Ayurvedic medicine, Reiki, and healing touch. Many treatments are self-selected due to minimal FDA regulation and over-the-counter availability. Herbs are the most common CAM products, especially popular for psychiatric disorders. Anxiety is a strong predictor of herbal remedy use,127 often used without physician knowledge. Clinicians and pharmacists should monitor all treatments patients use, including medication reconciliation of prescription and non-prescription products, herbs, and supplements at each visit.
Herbal trial results for anxiety disorders are mixed. Kava use for anxiolysis declined due to hepatotoxicity reports, leading to warnings and market withdrawal in many countries.128,129 However, a randomized trial of a benign aqueous formulation showed moderate anxiety symptom reduction in mixed anxiety disorder patients.128,130 St. John’s wort and milk thistle have been used for OCD symptoms, but placebo-controlled trials showed no significant differences.131,132 Lower-quality CAM studies report modest effects for mindfulness meditation, yoga, and acupuncture.133
Despite limited efficacy data, many patients continue CAM therapies, necessitating monitoring for interactions with prescription medications.134 St. John’s wort interacts with many drugs via CYP isoenzyme induction, potentially decreasing alprazolam and clonazepam levels and increasing serotonin syndrome risk with SSRIs. Milk thistle inhibits CYP3A4, potentially increasing levels of other medications metabolized by this pathway. Kava inhibits several CYP isoenzymes.135 Further research into alternative anxiety disorder strategies is needed.
Functional Status
While treatment can relieve anxiety symptoms, residual symptoms often impact daily function. Even subclinical anxiety can cause disability exceeding that of severe mental illnesses.111,136 Chronic, persistent anxiety disorders significantly impact lives, causing social and work skill deficits. Few interventions focus on rehabilitation and functional restoration.
Stress is key in anxiety syndrome emergence and maintenance. Return-to-work stress can trigger symptom re-emergence, decreasing productivity and potentially leading to job loss. More research is needed to address this problem.
CONCLUSION
Anxiety disorders are treatable. Effective treatments and refined algorithms exist. However, integrating biological mechanism knowledge with treatment is crucial for predicting and improving treatment response. Dynamic anxiety models like the ABC model aid in understanding symptom development and maintenance, and biological-psychological factor interplay.
Improving real-world administration of effective treatments, especially in primary care, and public education are vital. Continued testing of alternative therapies for anxiety treatment and prevention, and assisting patients with treatment-resistant anxiety are essential.
Addressing patient feelings about mental illness early in treatment is also important. These measures will enhance anxiety care.
Footnotes
Disclosure: Dr. Bystritsky reports honoraria, research grants, and travel reimbursements from AstraZeneca, Takeda, and Brainsway. He has consulted for UpToDate, John Wiley & Sons, Brainsonix Corp., and Consumer Brands. Dr. Khalsa, Dr. Cameron, and Dr. Schi3man report no financial or commercial relationships related to this article. This work was partially funded by a grant from the Saban Family Foundation.
