Introduction
Infertility, defined by the World Health Organization (WHO) as the inability to achieve a clinical pregnancy after 12 months or more of regular, unprotected intercourse, affects a significant portion of couples globally, estimated at 10%–15% of reproductive-age couples. [1] In India, the prevalence of primary infertility alone ranges from 3.9% to 16.8%, highlighting a substantial public health concern. [2] Sexually transmitted infections are a major contributor to infertility worldwide, particularly in developing nations, often leading to pelvic inflammatory disease (PID) and subsequent tubal damage. [3] Female factors are predominant in infertility cases (40%–55%), followed by male factors (30%–40%), combined factors (10%), and unexplained etiologies in approximately 10% of cases.
Diagnostic hysterolaparoscopy (DHL) has become an indispensable tool in the assessment of female infertility. It is considered the gold standard for evaluating tubal patency and offers a comprehensive, direct visualization of the uterine cavity, endometrium, tubal structure and function, and pelvic organs. Conditions often missed by routine clinical exams and ultrasound scans can be accurately diagnosed through DHL. Beyond diagnosis, DHL also allows for therapeutic interventions in certain identified pathologies. This article explores the crucial role of Dhl Diagnosis in evaluating female infertility, drawing on findings from a detailed study conducted in a tertiary care hospital.
Materials and Methods: A Retrospective Study on DHL Diagnosis
A retrospective study was carried out at the North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences (NEIGRIHMS) in Shillong, India, a tertiary care center. The study spanned two years, from July 2014 to July 2016, and included couples presenting with both primary and secondary infertility, aged 20 to 45 years. Notably, women over 40 with sufficient antimullerian hormone levels, who could potentially benefit from DHL, were also included. Seven patients in the 40–45 age group were part of the study (six with primary and one with secondary infertility). Primary infertility was defined as never having conceived, while secondary infertility referred to those with at least one prior conception, regardless of pregnancy outcome. The average duration of infertility was similar in both groups: 5.1 ± 2.2 years for primary and 4.9 ± 2.7 years for secondary infertility.
The study criteria included a minimum infertility duration of one year, consistent with standard definitions. There was no upper limit on infertility duration. Patients with abnormal hysterosalpingograms (HSG) were included, irrespective of other known infertility factors. HSG can produce false positives for bilateral tubal blockage due to uterine spasm caused by dye injection. Chromopertubation (CPT) during DHL can overcome this, offering the added benefit of tubal cannulation, although cannulation was not a study outcome. Therefore, DHL and CPT are routine protocols at the institute for HSG-diagnosed tubal blocks. Patients with abnormal HSG results (tubal block, hydrosalpinx, uterine anomaly) were included and confirmed via DHL, but the study did not directly compare HSG and DHL findings.
Patients with endocrine disorders causing chronic anovulation (like polycystic ovarian syndrome, hyperprolactinemia, thyroid disorders) and couples with semen analysis abnormalities were excluded. Patients with contraindications to laparoscopy were also not included. DHL with CPT was performed during the preovulatory phase (days 6–12 of the menstrual cycle). Transvaginal sonography was not routinely performed before DHL, but if done, it was mainly for antral follicle count assessment. Patient selection was primarily based on abnormal HSG reports (tubal block, hydrosalpinx, uterine anomaly).
DHL was conducted under general anesthesia between days 6 and 11 of the menstrual cycle, using a 7mm Karl Storz laparoscope with a 30° angle telescope. Hysteroscopy was performed first, examining the vagina and cervix for abnormalities, and the uterine cavity for septa, congenital malformations, synechiae, polyps, fibroids, and endometrial condition. Tubal ostia patency was also assessed.
Following hysteroscopy, pneumoperitoneum was created, and laparoscopy was performed. The fallopian tubes, ovaries, pelvic peritoneum, pouch of Douglas, and peritoneal cavity were meticulously examined. Laparoscopic inspection included the uterus (shape, size, position, surface, fibroids), cul-de-sac (adhesions, obliteration, endometriosis, fluid), ovaries (size, shape, surface, cysts, tube relation), and fallopian tubes (size, shape, surface, kinking, dilatation, stricture, hydrosalpinx). Any features indicative of infertility were noted.
Finally, CPT was performed to evaluate tubal patency. Methylene blue dye was injected using a 20ml syringe through a Leech Wilkinson cannula or a 14F Foley catheter inserted into the uterine cavity (balloon inflated with 5ml saline). Dye spillage from the fimbrial end of the tubes was observed.
Statistical analysis was performed using SPSS software (version 22.0). Student’s t-tests and Chi-square tests were used to compare continuous variables and proportions, respectively.
Results: Key Findings from DHL Diagnosis
The study included 151 patients undergoing DHL, with 88 (58.28%) experiencing primary infertility and 63 (41.72%) secondary infertility. The average age of patients with primary infertility was 27.2 ± 2.6 years, and for secondary infertility, 32.4 ± 2.2 years. The duration of infertility was statistically similar in both groups [Table 1].
Table 1. Duration of infertility
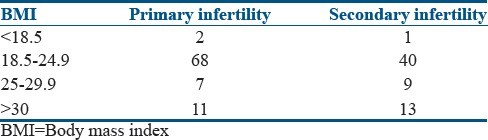
Dyspareunia history was reported by 17 patients with primary and 11 with secondary infertility. Body mass index (BMI) varied across groups [Table 2]. In the primary infertility group, two were underweight, seven overweight, and 11 obese. In the secondary infertility group, one was underweight, nine overweight, and 13 obese. Prior infertility treatments were also noted [Table 3]. In the primary infertility group, 22 had ovulation induction history, and nine had intrauterine insemination (IUI). For secondary infertility, 17 had ovulation induction and 11 IUI history. None had undergone in vitro fertilization (IVF) previously.
Table 2. Body mass index (BMI)
Table 3. Previous treatment history
Laparoscopic abnormalities were more prevalent than hysteroscopic findings in both primary (37.5% vs 7.95%) and secondary (49.2% vs 14.29%) infertility patients [Table 4]. Laparoscopic abnormalities were significant in both groups. Thirteen primary and five secondary infertility patients had multiple abnormal findings during DHL. The most common laparoscopic abnormalities in both groups were indicative of PID, specifically adnexal adhesions and hydrosalpinx [Table 5]. Findings suggestive of tuberculosis (TB), such as caseous material and tubercles, were observed in six primary and three secondary infertility patients (TB later confirmed by PCR). Uterine synechiae was the most frequent hysteroscopic abnormality [Table 6]. Cervical stenosis was found in one primary infertility patient, and an arcuate uterus in one secondary infertility patient. Tubal block was more common in primary than secondary infertility [Table 7], with bilateral blocks being more frequent than unilateral ones.
Table 4. Prevalence of hysteroscopic and laparoscopic abnormalities
Table 5. Laparoscopy findings
Table 6. Hysteroscopy findings
Table 7. Prevalence of tubal block (chromopertubation test)
Patients generally tolerated the procedure well, with mild postoperative abdominal pain being the only common complaint. No major complications occurred.
Discussion: Understanding the Diagnostic Value of DHL
Infertility poses significant emotional, social, and financial challenges for couples. Among female infertility factors, tuboperitoneal pathology is a leading cause, accounting for 30%–35% of cases, followed by ovulatory dysfunction (20%–30%) and uterine pathology (15%). [4, 5] Laparoscopy is the established gold standard for evaluating tuboperitoneal pathology. [6] This study’s findings align with this, as pelvic adhesions and hydrosalpinx were the most frequent tubopelvic pathologies observed during laparoscopy. Adnexal adhesions are a well-known indicator of PID. [7] Hydrosalpinx is commonly caused by PID and pelvic tuberculosis. [8] Hydrosalpinx is significantly linked to infertility and poorer IVF outcomes. [9] PID prevalence in India ranges from 1% to 17%. [10] Even subclinical PID can significantly impair fertility, with affected women experiencing approximately 40% fewer pregnancies compared to those without. [11] Tubal factor infertility, largely due to PID, is a primary cause of female infertility. [12] In addition to hydrosalpinx, the study also identified features suggestive of TB, such as caseous material and tubercles, in some patients. Genital TB prevalence in women varies from 1% to 19% depending on the region. [13] An Indian study found genital tuberculosis in over 25% of infertile women (40 out of 150). [14]
Endometriosis was found in 9.3% of patients during laparoscopy in this study, manifesting as endometriomas, nodules, and powder burn lesions. Laparoscopy remains the gold standard for diagnosing endometriosis through direct visualization. [15] It’s estimated that 30%–50% of women with endometriosis experience infertility. [16]
Uterine fibroids (myomas) were detected in 6% of patients during laparoscopy and 1.99% during hysteroscopy. Among fibroid cases in the primary infertility group, four were submucosal and three intramural. In the secondary infertility group, two were intramural and one submucosal. Pritts et al. concluded that submucosal fibroids (FIGO L0–L2), which distort the uterine cavity, are associated with decreased clinical pregnancy, implantation, and live birth rates, and increased miscarriage rates. [17] Their review also indicated that intramural fibroids (FIGO L3–L4) without submucosal involvement are linked to reduced implantation and live birth rates, and higher miscarriage rates, compared to controls without fibroids. [18] Subserosal fibroids (FIGO L5–L7) were not found to negatively impact fertility measures. [17]
Uterine anomalies are present in about 8% of infertile women, with septate uterus being the most common. Arcuate uterus is the most frequent anomaly in the general population and is not specifically linked to increased infertility risk. [18] In this study, uterine anomalies were found in 1.3% of laparoscopy patients and 1.99% of hysteroscopy patients, predominantly septate and arcuate uterus.
Intrauterine adhesions (Asherman syndrome) are a rare but significant cause of menstrual irregularities and infertility. [19] In India, genital tuberculosis is a significant cause of Asherman syndrome, unlike in developed countries. [20] Intrauterine adhesions were the most common hysteroscopic finding in this study.
Tubal block was observed in 17.9% of patients unilaterally and 37.7% bilaterally in this study. The high prevalence of tubal block in this study could be attributed to the hospital being a tertiary referral center, where many patients are referred with pre-diagnosed tubal blocks from HSG.
Postoperative recovery was generally smooth, with mild pain manageable with analgesics. No major complications were observed.
Conclusion: The Continued Importance of DHL in Infertility Diagnosis
Diagnostic hysterolaparoscopy remains a valuable procedure for identifying and potentially treating reversible causes of infertility, such as adnexal adhesions, tubal blockages, and uterine synechiae. Even with advancements in ultrasound technology, DHL diagnosis continues to offer hope for many infertile couples, especially in developing countries, by providing detailed diagnostic information crucial for effective fertility management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
[1] Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. Hum Reprod Update 2012;18:485-501.
[2] Datta J, Palmer MJ, Tanton C, Gibson LJ, Saunders D, Shantikumar S, et al. National and regional prevalence of infertility in India: a systematic review and meta-analysis. Hum Reprod Update 2016;22:546-59.
[3] World Health Organization. Sexually transmitted infections (STIs). Fact sheet No. 110. Reviewed January 2018. Available from: http://www.who.int/mediacentre/factsheets/fs110/en/. [Last accessed on 2018 Feb 23].
[4] Rowe PJ, Comhaire FH, Hargreave TB, Mahmoud AM. WHO manual for the standardized investigation, diagnosis and management of the infertile couple. Cambridge: Cambridge University Press; 2000.
[5] Hull MG, North K, Taylor H, Farrow A, Ford WC. Population study of causes, treatment, and outcome of infertility. Br Med J (Clin Res Ed) 1985;291:1693-7.
[6] Brosens I, Gordts S, Campo R, Puttemans P, Benagiano G. Hysteroscopy: past, present, future. Best Pract Res Clin Obstet Gynaecol 2010;24:75-91.
[7] Weström L. Pelvic inflammatory disease: bacteriology and sequelae. Contraception 1987;36:Suppl:141-53.
[8] Sharma JB, Roy KK, Pushparaj M, Kumar S, Malhotra N, Mittal S. Genital tuberculosis amongst women attending infertility clinic: revised diagnostic and management strategies. Indian J Med Res 2009;130:593-8.
[9] Johnson N, van Voorst Vader PC, Farquhar C, Bhattacharya S,ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়ীয়