Introduction
Acute gastroenteritis (AGE), a common illness globally, particularly affects children and poses a significant health burden. Rotavirus is a leading cause of AGE in young children worldwide. Accurate diagnosis and coding of AGE are crucial for epidemiological studies, vaccine impact assessments, and public health surveillance. This article delves into the complexities of diagnosis codes for acute gastroenteritis, focusing on the International Classification of Diseases, Tenth Revision (ICD-10) and its implications for research and public health practice. Understanding the nuances of these codes, particularly in the context of evolving coding directives, is essential for healthcare professionals and researchers alike.
Background: The Importance of ICD-10 Codes in AGE Diagnosis
The International Classification of Diseases (ICD) is a globally recognized system for classifying diseases and health problems. The ICD-10, the tenth revision, is widely used for diagnostic coding in healthcare settings and for statistical reporting. In the context of acute gastroenteritis, ICD-10 codes are used to categorize different types of AGE based on etiology (cause) and clinical presentation. These codes are instrumental in various aspects of healthcare and research, including:
- Epidemiological Studies: ICD-10 codes enable researchers to track the incidence and prevalence of AGE, identify trends, and monitor outbreaks.
- Vaccine Impact Assessments: For diseases like rotavirus AGE, ICD-10 codes are vital for evaluating the effectiveness of vaccination programs by measuring reductions in AGE-related hospitalizations and emergency department visits.
- Public Health Surveillance: Consistent and accurate coding using ICD-10 allows for effective surveillance of infectious diseases and informs public health interventions.
- Clinical Management: While not directly used for immediate patient care, ICD-10 codes contribute to a standardized system for documenting diagnoses, which aids in long-term patient record keeping and healthcare system analysis.
Historically, studies assessing the impact of interventions like rotavirus vaccines have heavily relied on administrative health data, which uses ICD codes to identify cases of AGE. This approach necessitates a clear understanding of the specific ICD-10 codes used for AGE and how changes in coding guidelines can affect data interpretation.
 ICD-10 Classification System for Gastroenteritis
ICD-10 Classification System for Gastroenteritis
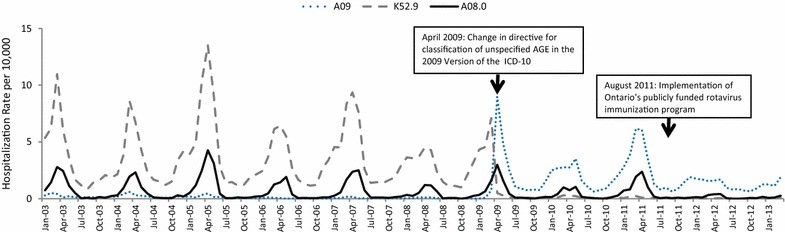
Image alt text: Temporal trends in hospitalizations for acute gastroenteritis among Ontario children aged 0 to 15 years, using select ICD-10-CA codes, illustrating the impact of coding directive change in 2009.
The 2009 ICD-10 Coding Directive Change: A Critical Shift
A significant change in the ICD-10 coding directive occurred in 2009, impacting how unspecified gastroenteritis cases were classified. Prior to 2009, the guideline in some regions, including Canada’s ICD-10-CA modification, was to “assume gastroenteritis to be noninfectious unless documented as infectious by the responsible physician.” This meant that cases of gastroenteritis not specifically identified as infectious were coded under K52.9, representing “Noninfective gastroenteritis and colitis, unspecified.”
However, in 2009, the World Health Organization (WHO) issued a revised directive, reflected in the ICD-10 Version 2009 and subsequent updates, stating that “most cases of gastroenteritis are infectious, even in industrialized countries, thus ICD-10-CA version 2009 classifies gastroenteritis not otherwise specified (NOS) as infectious (A09.9 Gastroenteritis and colitis of unspecified origin).” This change meant that unspecified gastroenteritis cases, previously coded as non-infectious (K52.9), were now to be classified as infectious (A09.9).
This shift had a profound impact on the interpretation of epidemiological data, particularly for studies spanning the 2009 period. An apparent increase in reported infectious gastroenteritis (A09) and a decrease in non-infectious gastroenteritis (K52.9) after 2009 might not reflect a true change in disease incidence, but rather a change in coding practice.
Investigating the Coding Change: A Case Study in Ontario, Canada
To illustrate the impact of this coding change, let’s consider a study conducted in Ontario, Canada, evaluating the impact of rotavirus vaccine on hospitalizations and emergency department (ED) visits for AGE. Initially, researchers used a set of ICD-10-CA codes to identify AGE cases, including:
- A08.0: Rotaviral enteritis (RV-specific AGE)
- A08.3: Other viral gastroenteritis
- A08.4: Viral intestinal infection, unspecified
- A08.5: Other specified intestinal infections
- A09: Other gastroenteritis and colitis of infectious and unspecified origin
Upon analyzing data from January 2003 to March 2013, an unexpected increase in AGE hospitalizations, particularly coded as A09, was observed starting in April 2009. This increase coincided precisely with the implementation of the new ICD-10 coding directive. Further investigation revealed that cases previously coded under K52.9 were now being classified under A09.9 due to the directive change.
To account for this, the researchers modified their outcome definition to include K52.9 (“Noninfective gastroenteritis and colitis, unspecified”) in addition to the original set of codes. This adjustment provided a more accurate picture of AGE trends, mitigating the artificial inflation of A09 cases post-2009.
Image alt text: Seasonal variation in hospitalizations for acute gastroenteritis among Ontario children aged 0 to 15 years, illustrated with two case definitions using ICD-10 diagnostic codes, highlighting the impact of including or excluding code K52.9.
Implications for Rotavirus Vaccine Impact Studies and Future Research
The 2009 ICD-10 coding change has significant implications for studies evaluating the impact of rotavirus vaccines and other interventions aimed at reducing AGE burden. Researchers must be acutely aware of this change, especially when analyzing data spanning the pre- and post-2009 periods.
Recommendations for Researchers:
- Include both A09.9 and K52.9: For studies covering periods that include or extend beyond 2009, it is crucial to include both A09.9 and K52.9 ICD-10 codes in the outcome definition to capture all unspecified cases of AGE, regardless of the coding directive in place.
- Stratified Analysis: Consider analyzing data stratified by time periods before and after April 1, 2009, to assess the potential impact of the coding change on observed trends.
- Sensitivity Analysis: Perform sensitivity analyses using different outcome definitions (e.g., with and without K52.9) to evaluate the robustness of study findings to coding variations.
- Consult Coding Guidelines: Researchers should consult the specific ICD-10 coding guidelines applicable to their study region and time period to fully understand potential coding changes and their implications.
- Transparency in Methods: Clearly document the ICD-10 codes used for outcome ascertainment and acknowledge the potential influence of coding directive changes in study methodology sections.
By carefully considering the 2009 ICD-10 coding change, researchers can ensure more accurate and reliable assessments of rotavirus vaccine impact and other public health interventions. Failing to account for this change could lead to misinterpretations of data and potentially flawed conclusions about disease trends and intervention effectiveness.
Conclusion: Navigating Diagnosis Codes for Accurate AGE Assessment
Understanding the diagnosis codes for acute gastroenteritis, particularly within the ICD-10 framework, is essential for accurate epidemiological research, vaccine impact evaluation, and public health surveillance. The 2009 ICD-10 coding directive change regarding unspecified gastroenteritis serves as a critical example of how modifications in coding practices can significantly affect data interpretation. Researchers and healthcare professionals must remain vigilant about such changes and adapt their methodologies to ensure data accuracy and validity. For studies involving AGE and utilizing ICD-10 codes, especially those spanning 2009, the inclusion of both A09.9 and K52.9 codes is a recommended best practice to comprehensively capture unspecified AGE cases and avoid potential biases introduced by coding directive shifts. By paying close attention to these coding nuances, we can improve the quality and reliability of research and surveillance efforts related to acute gastroenteritis, ultimately contributing to better public health outcomes.
References
- Reference 1 from original article
- Reference 2 from original article
- Reference 3 from original article
- Reference 4 from original article
- Reference 5 from original article
- Reference 6 from original article
- Reference 7 from original article
- Reference 8 from original article
- Reference 9 from original article
- Reference 10 from original article
- Reference 11 from original article
- Reference 12 from original article
- Reference 13 from original article
- Reference 14 from original article
- Reference 15 from original article
- Reference 16 from original article
- Reference 17 from original article
- Reference 18 from original article
- Reference 19 from original article
- Reference 20 from original article
- Reference 21 from original article
- Reference 22 from original article
- Reference 23 from original article
- Reference 24 from original article
- Reference 25 from original article
- Reference 26 from original article
- Reference 27 from original article