Chronic diarrhea, defined as persistent diarrhea lasting four weeks or more, is a prevalent condition affecting approximately 5% of the global population across all demographics. This condition significantly impacts patient well-being and quality of life, posing substantial economic burdens on healthcare systems due to its complex diagnosis and management. The Differential Diagnosis For Chronic Diarrhea is extensive, encompassing a wide array of etiologies from infections and endocrine disorders to malabsorption syndromes and gut-brain interaction disorders. The overlapping nature of symptoms across these diverse conditions often complicates accurate diagnosis, leading to potential delays and misdiagnoses. This article provides an in-depth review of the differential diagnosis of chronic diarrhea, with a particular focus on Irritable Bowel Syndrome with Diarrhea (IBS-D) and Exocrine Pancreatic Insufficiency (EPI). These two conditions, while presenting with similar symptoms, have distinct underlying causes and necessitate vastly different management approaches. We will outline a structured four-step diagnostic strategy and propose a clear algorithm designed to efficiently differentiate IBS-D from EPI and other causes of chronic diarrhea. Our aim is to enhance diagnostic precision, ultimately improving patient quality of life and reducing the healthcare burden associated with this common ailment.
Key Words: Chronic Diarrhea, Differential Diagnosis, Irritable Bowel Syndrome with Diarrhea (IBS-D), Exocrine Pancreatic Insufficiency (EPI), Diagnostic Algorithm
Chronic diarrhea, characterized by diarrhea lasting longer than four weeks, is a common health issue affecting up to 5% of individuals globally, irrespective of age, gender, ethnicity, or socioeconomic background.1 A recent worldwide internet survey spanning 25 countries revealed that functional diarrhea was reported by 4.7% of the 54,127 participants.2 The human and economic costs associated with diarrhea are substantial, resulting in diminished health-related quality of life, disruption of daily routines, and a significant increase in the use of healthcare resources.3,4 Peery et al. highlighted the burden and expenses of gastrointestinal illnesses in the United States, indicating over 36.8 million outpatient visits for gastrointestinal symptoms and 43.4 million visits with a primary gastrointestinal diagnosis in 2016.5 Diarrhea ranked as the fourth most frequent gastrointestinal symptom prompting outpatient healthcare visits (office and emergency department; n=2,583,060) and the sixth most common gastrointestinal physician diagnosis (n=1,988,413).5
The differential diagnosis of chronic diarrhea is broad and diverse, including infectious agents (e.g., bacterial, parasitic, viral), endocrine disorders (e.g., hyperthyroidism, diabetes), maldigestion and malabsorption disorders (e.g., celiac disease, lactose intolerance, exocrine pancreatic insufficiency [EPI]), disorders of gut-brain interaction (e.g., irritable bowel syndrome [IBS]), inflammatory conditions (e.g., Crohn’s disease, ulcerative colitis), secondary factors like medications (e.g., laxatives), and toxic substance ingestion (e.g., alcohol abuse).6,7 The symptom overlap among these numerous conditions often complicates accurate diagnosis. Consequently, patients may experience diagnostic delays or misdiagnosis, leading to persistent symptoms and other adverse outcomes.8–12 Therefore, efficient and accurate diagnosis is crucial.
This review aims to provide a comprehensive strategy for differentiating and accurately diagnosing the wide range of diarrhea-related illnesses encountered in clinical practice, with a focus on IBS with diarrhea (IBS-D) and EPI. We explore the optimal methods for distinguishing IBS-D and EPI from each other and from other conditions with similar presentations. This approach aims to facilitate earlier and more precise diagnoses, leading to improved treatment, enhanced quality of life, and more efficient utilization of healthcare resources.
IRRITABLE BOWEL SYNDROME: A Key Cause of Chronic Diarrhea
Irritable Bowel Syndrome (IBS) stands as the most prevalent cause of diarrhea in developed countries, with an estimated prevalence of 4% to 9% in the United States, based on Rome III/IV criteria.13,14 While IBS can manifest at any age, it is most commonly diagnosed in women aged 20 to 40, with women being diagnosed approximately twice as frequently as men (14% vs. 8.9%).15
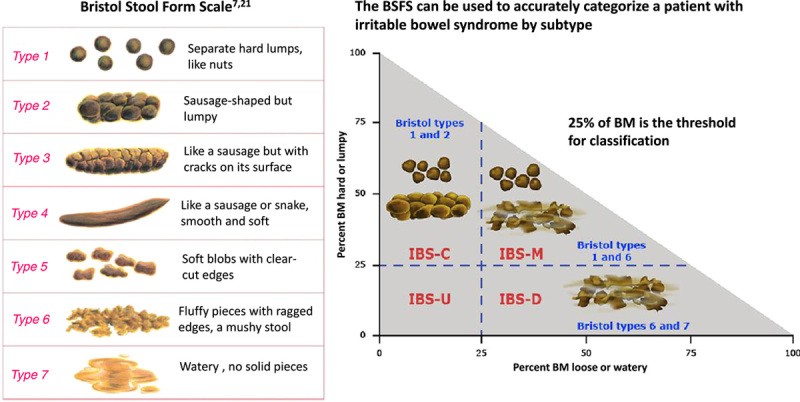
According to the Rome IV clinical diagnostic criteria, IBS can be diagnosed if a patient experiences recurrent abdominal pain, on average, at least one day per week, associated with changes in visceral sensation related to defecation and/or alterations in stool form or frequency. These symptoms must also impact the patient’s quality of life or their ability to perform daily activities. Although the clinical criteria do not specify a duration for symptom presence, it is essential for the healthcare provider to confidently exclude other potential diagnoses. The Rome IV research-based criteria are more stringent, requiring symptoms to be present for the preceding three months with symptom onset at least six months prior to diagnosis (Table 1).7,17 Symptoms commonly observed in IBS-D patients, although not included in the core definition, include abdominal bloating and distension, fecal urgency, a sensation of incomplete evacuation, and mucus in stools.7 Stools are typically watery, corresponding to Bristol Stool Form Scale 6-7 (Fig. 1), and bowel movements occur during waking hours. Stress is a recognized contributing factor.6,18 Crucially, certain ‘red flags’ or alarm features necessitate further investigation for organic causes of diarrhea rather than IBS. These include symptom onset in individuals older than 50 years, unintentional weight loss, sudden unexplained changes in symptoms, recurrent rectal bleeding or anemia, and a family history of inflammatory bowel disease, celiac disease, or colorectal cancer (Figs. 2 and 3).
TABLE 1. Rome IV Diagnostic Criteria for Irritable Bowel Syndrome
| Clinical diagnostic criteria | Research diagnostic criteria |
|---|---|
| Recurrent abdominal pain on average at least 1 day/week, associated with two or more of the following criteria*: Related to defecation Associated with a change in frequency of stool Associated with a change in form (appearance) of stool Bothersome symptoms: Interfere with daily activities Require attention Cause worry or interfere with the quality of life | Recurrent abdominal pain on average at least 1 day/week in the last 3 mo, associated with two or more of the following criteria†: Related to defecation Associated with a change in frequency of stool * Associated with a change in the form (appearance) of stool |
*For the last 8 weeks.
†For the last 3 months with symptom onset at least 6 months before diagnosis.
FIGURE 1. Bristol Stool Form Scale and IBS Subtypes
Alt Text: Bristol Stool Chart illustrating stool types 1 through 7, with types 6 and 7 indicating diarrhea, relevant for diagnosing Irritable Bowel Syndrome with Diarrhea (IBS-D) and differentiating stool consistency.
FIGURE 2. General Sequence for Differential Diagnosis of Chronic Diarrhea
Alt Text: Flowchart outlining a general diagnostic sequence for chronic diarrhea, including initial assessment, alarm feature evaluation, and targeted testing for conditions like celiac disease, Inflammatory Bowel Disease (IBD), Irritable Bowel Syndrome with Diarrhea (IBS-D), and Exocrine Pancreatic Insufficiency (EPI).
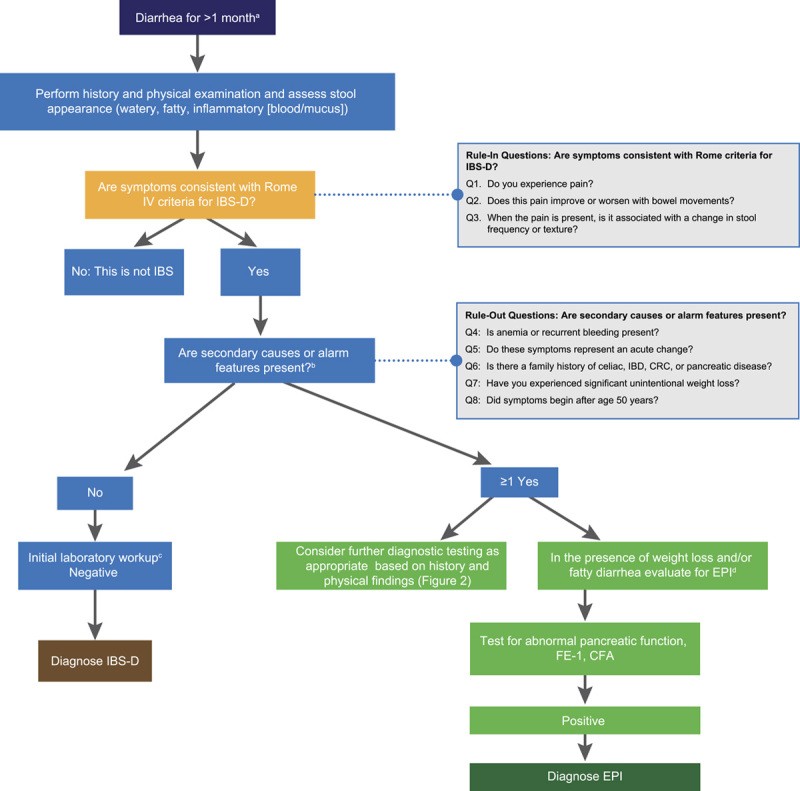
FIGURE 3. A General Strategy for Differential Diagnosis: EPI or IBS-D?
Alt Text: Diagnostic algorithm designed to differentiate between Exocrine Pancreatic Insufficiency (EPI) and Irritable Bowel Syndrome with Diarrhea (IBS-D) in patients presenting with chronic diarrhea, incorporating Rome IV criteria and alarm symptoms.
While chronic abdominal pain is a defining symptom differentiating IBS from functional diarrhea, a significant overlap exists between these two conditions, and patients may fluctuate between diagnoses.19,20 Patients with IBS, particularly those experiencing frequent pain, exhibit increased psychological distress and somatic comorbidities compared to those with functional diarrhea, necessitating appropriate evaluation. Early intervention in these overlapping conditions can be beneficial.21
Currently, there is no universally accepted biomarker for IBS diagnosis, and extensive testing to rule out organic causes is generally discouraged due to high costs, inefficiency, and low diagnostic yield.19,22,23 In many cases, an accurate IBS diagnosis can be achieved based on subjective patient history alone. A retrospective study by Vanner et al.24 demonstrated that Rome Criteria for IBS, in the absence of alarm symptoms, had specificity and positive predictive values of 100%. None of the patients diagnosed with IBS required a revised diagnosis within two years. Prospective analyses have shown positive predictive values approaching 98%.24 Consequently, clinical guidelines recommend minimizing diagnostic investigations and adopting a positive diagnostic strategy.16,19,25 The American College of Gastroenterology (ACG) and American Gastroenterological Association (AGA) advise against routine colonoscopy, except for patients over 45 years of age (for age-appropriate screening) or those with warning signs of more serious illness.16,22,26
Recommended diagnostic tests are limited and include serologic testing to exclude celiac disease (specifically serum IgA and tissue transglutaminase IgA), fecal calprotectin (or lactoferrin), and C-reactive protein in patients without clinical signs suggestive of more serious disease to rule out inflammatory bowel disease. Giardia stool antigen testing is recommended for individuals with a history of travel to or emigration from endemic regions, exposure to untreated water, or contact in daycare settings.16
Irritable Bowel Syndrome Subtypes and IBS-D
Irritable bowel syndrome is classified into four subtypes based on predominant stool patterns: IBS-D (diarrhea-predominant), IBS-C (constipation-predominant), IBS-M (mixed bowel habits), and IBS-U (unclassified).7,8 Among these, IBS-D is the most common, affecting up to 40% of adults diagnosed with IBS.27 Globally, 1.2% of individuals experience IBS-D, with a slight female predominance (1.3% vs. 1.0% in males).2
Patients with IBS-D typically pass Bristol Stool Form Scale type 6 or 7 stools (loose, mushy, watery) in more than 25% of bowel movements and types 1 and 2 stools (hard, lumpy, pellet-like) less than 25% of the time (Fig. 1).7,19 Rome IV diagnostic criteria specify that stool texture assessment should be performed on days with abdominal pain to enhance the precision of IBS subtype differentiation.7,28
Due to symptom overlap with other conditions like EPI, celiac disease, small intestinal bacterial overgrowth, disaccharidase deficiencies, Crohn’s disease, ulcerative colitis, and infections, diagnosing IBS-D can be challenging.17 However, initial categorization of diarrhea as watery (suggestive of IBS), fatty or greasy (suggestive of EPI), or inflammatory (suggestive of inflammatory bowel disease) can help narrow the differential diagnosis (Table 2).6
TABLE 2. Narrowing the Diagnosis Based on Stool Characteristics
| Watery Diarrhea | Fatty/Greasy Diarrhea | Inflammatory Diarrhea |
|---|---|---|
| Osmotic: Carbohydrate malabsorption Celiac disease Osmotic laxatives Secretory: Bile acid malabsorption Microscopic colitis Endocrinopathies (e.g., diabetes, hyperthyroidism) Medications (e.g., metformin) Functional: Functional diarrhea * Irritable bowel syndrome | Malabsorption or Maldigestion: Celiac disease Small intestinal bacterial overgrowth Giardiasis Whipple disease Inadequate luminal bile acid concentration Exocrine pancreatic insufficiency | Inflammatory Bowel Disease: Segmental colitis associated with diverticulosis (SCAD) Infectious Disease: Clostridium difficile Invasive bacterial infections Invasive parasitic infections Other: Ischemic colitis Radiation colitis * Lymphoma |
EXOCRINE PANCREATIC INSUFFICIENCY: An Important Differential
Exocrine Pancreatic Insufficiency (EPI), while commonly linked to pancreatic diseases, can also result from various extrapancreatic conditions.29 Approximately 80% of children with cystic fibrosis develop EPI within the first two years of life,30 and EPI affects 10% to 30% of patients with mild and 85% with severe chronic pancreatitis.30,31 Among patients with pancreatic cancer, about 72% develop EPI, with a significantly higher incidence (3.36 times) when the tumor is located in the pancreatic head compared to the body or tail.32 In pancreatic diseases, reduced pancreatic enzyme and bicarbonate secretion occurs due to parenchyma dysfunction and/or obstruction of the main pancreatic duct.33
EPI is characterized by a deficiency in the quantity or activity of pancreatic enzymes in the intestinal lumen, leading to impaired food digestion.29,34,35 Inadequate fat digestion is the most clinically relevant consequence of EPI.30 Diarrhea in EPI develops when the digestive capacity of the exocrine pancreas is overwhelmed by the quantity and quality of ingested food. Symptom prevalence in EPI patients varies considerably, primarily due to differing dietary habits and restrictions. Clinical studies in confirmed EPI patients reported clinically evident steatorrhea (fatty/oily loose stools) in 23% to 70% of chronic pancreatitis cases, 46% of preoperative pancreatic cancer patients, and 15% of cystic fibrosis patients.36 A detailed patient history is crucial, as dietary restrictions can confound diagnosis. For instance, a low-fat diet, adopted to manage symptoms, may mask EPI symptoms, making diagnosis challenging in asymptomatic patients.36
EPI patients typically present with symptoms of malabsorption syndrome, including diarrhea, abdominal distension and cramps, flatulence, weight loss, and nutritional deficiencies (fat-soluble vitamins, micronutrients, proteins).33,34,37 Symptom severity varies based on the underlying cause, enzyme deficit, and fat intake. Common patient reports include foul-smelling, fatty, loose stools; flatulence; and weight loss.37 Long-term consequences of EPI include sarcopenia, osteoporosis, low-trauma fractures, metabolic bone disease (especially in chronic pancreatitis), increased infection risk, and cardiovascular disease.30,34,35,38,39
EPI should be considered in chronic diarrhea patients with a history of pancreatic disease (acute, relapsing, or chronic pancreatitis; cystic fibrosis; pancreatic cancer; acute necrotizing pancreatitis; and type 1, 2, or 3c diabetes mellitus), risk factors for pancreatic disease (alcohol abuse and/or smoking), family history of pancreatic diseases (mainly chronic pancreatitis or pancreatic cancer), or pancreatic or gastric surgery.32,33 EPI testing is warranted in patients without a history of pancreatic disease only when clinical suspicion is high.
Definitive EPI diagnosis is often challenging due to the lack of highly accurate tests, but it is crucial to prevent complications. Diagnosis typically involves a combination of symptom assessment, nutritional marker evaluation, and non-invasive pancreatic function tests, such as coefficient of fat absorption (CFA) and fecal elastase (FE-1).30,33,34 While other pancreatic function tests exist, they are either invasive (e.g., endoscopic pancreatic function test [ePFT]) or not widely accessible (e.g., 13C-labeled breath tests) for routine clinical use.37 The direct secretin-cholecystokinin (CCK) test is the most sensitive for detecting reduced stimulated pancreatic secretion but is invasive, expensive, cumbersome, and time-consuming, limiting its clinical utility.40 The ePFT after intravenous secretin administration was developed as an alternative but still has limitations.41,42 Both the secretin-CCK test and ePFT are primarily used for functional diagnosis of chronic pancreatitis in cases with inconclusive imaging and are not ideal for EPI diagnosis.40,43
The CFA test is considered the gold standard for EPI diagnosis,34,37 but its complexity limits its practical use. It requires patients to consume a diet with 100 g of fat/day for five days and collect total fecal output from days 3 to 5 for laboratory analysis. This procedure is cumbersome, unpleasant, and difficult for patient compliance, resulting in its rare use in clinical practice.36,37 13C-labeled breath tests offer an accurate and standardized alternative to CFA for EPI diagnosis in clinical settings but are not yet widely available.44,45 Fecal elastase-1 (FE-1) test measures the concentration of pancreatic-specific elastase in a small stool sample, reflecting pancreatic enzyme secretion.46 The FE-1 test is simple, widely available, and frequently used for pancreatic function assessment.37 The optimal cutoff and accuracy of FE-1 for EPI diagnosis, using CFA as the gold standard, vary across studies. Using optimal cutoffs ranging from 84 to 200 µg/g, FE-1 sensitivity ranges from 68% to 94%, and specificity from 48% to 82%.46–50
In chronic diarrhea patients with a high likelihood of EPI (e.g., pancreatic cancer in the head, advanced chronic calcifying pancreatitis, pancreatic surgery), pancreatic function tests are of limited diagnostic value and not necessary for diagnosis. In patients with chronic diarrhea but low EPI probability (e.g., no prior pancreatic disease or surgery, no risk factors, no weight loss or nutritional deficiencies), normal FE-1 levels rule out EPI. Low FE-1 levels may suggest EPI, warranting pancreatic investigation, but false-positive FE-1 results are not uncommon.46
EPI is among the organic gastrointestinal diseases that can mimic IBS.12,51 EPI, defined by low FE-1 concentration, is present in 5% to 6% of patients meeting Rome criteria for IBS-D and 4.6% of patients with unexplained abdominal pain and/or diarrhea and/or IBS-D.12,23,52 However, due to the possibility of false-positive FE-1 results in watery diarrhea, low FE-1 levels do not definitively exclude IBS-D.
DIFFERENTIAL DIAGNOSIS OF CHRONIC DIARRHEA: A Step-by-Step Approach
Early and accurate diagnosis is vital in managing chronic diarrhea. Patients may exhibit a range of symptoms indicative of various disorders, including IBS-D, EPI, celiac disease, small intestinal bacterial overgrowth, inflammatory bowel disease, and infections. Common symptoms such as diarrhea, abdominal pain, bloating, and flatulence are shared across these conditions. To aid in accurate diagnosis, we propose a four-step diagnostic process (Fig. 2).
Step 1: Comprehensive History and Physical Examination
Diagnosis should commence with a thorough history and physical examination.6,10,53 Patients presenting with chronic diarrhea (lasting ≥4 weeks) should be questioned in detail about their symptoms and diarrhea history.10,18,54 While the clinical definition of diarrhea is loose or watery stools ≥3 times in 24 hours,1,18 patients may use varying descriptions (e.g., loose stools, increased stool frequency, fecal urgency), highlighting the importance of a precise and detailed patient history.54 Abnormal stool form is often more critical in defining diarrhea, as patients with functional constipation can also report diarrhea due to increased defecation frequency, but further questioning may reveal symptoms of straining, incomplete evacuation, obstruction, and hard stools.1,55
Initially, we recommend categorizing diarrhea as watery (suggestive of IBS, celiac disease, endocrinopathy, or laxative misuse), fatty or greasy (suggestive of malabsorption or maldigestion like celiac disease or EPI), or inflammatory (suggestive of infectious or inflammatory bowel disease).6 However, definitive categorization can be challenging due to symptom overlap (Table 2). Further inquiries should address: diarrhea pattern (continuous, intermittent, meal-related – differentiating secretory from osmotic diarrhea), onset, precipitating events, stool volume, presence of blood, mucus, or fat, nocturnal diarrhea, and fecal urgency or incontinence.10,53,54,56 Additionally, explore other gastrointestinal and extraintestinal symptoms, potential aggravating factors (diet, stress, medications),10,18,56 and alleviating factors.10,53
Step 2: Identifying Risk Factors, Iatrogenic Factors, and Prior Diagnoses
To exclude extrinsic causes of chronic diarrhea, assess for recent travel (to regions with specific diarrhea-related pathogens like Giardia), gastrointestinal surgery (e.g., gallbladder removal, ileocecal resection, Roux-en-Y gastric bypass), radiation therapy, or diarrhea-inducing medications. Pre-existing mucosal (e.g., celiac disease), hepatic, pancreaticobiliary, neoplastic, or systemic (endocrine, vascular, or immunologic) diseases can also increase diarrhea risk.6,10,53,56
Step 3: Ruling Out Alarm Features
Several clinical features suggest more serious underlying conditions. It is crucial to rule out alarm features such as recent onset (especially in older patients), nocturnal diarrhea, severe or worsening symptoms, unexplained weight loss, family history of gastroenterological or systemic diseases (celiac disease, inflammatory bowel disease, colorectal cancer), blood in stool, and unexplained iron deficiency.6,53,56
Step 4: Initial Laboratory Workup
History and physical examination findings should guide the diagnostic strategy. If alarm signs or symptoms are present, testing should target the most likely etiologies. For instance, in patients with chronic meal-related fatty-greasy diarrhea, weight loss, and fat-soluble vitamin deficiencies, EPI workup is warranted. FE-1 level measurement is the most common indirect test for exocrine pancreatic function; FE-1 levels <200 µg/g suggest EPI.29,57 However, in patients with symptoms consistent with functional diarrhea or IBS-D (without alarm signs/symptoms), recent AGA and ACG guidelines recommend screening for celiac disease (anti-tissue transglutaminase IgA and total IgA), inflammatory bowel disease (fecal calprotectin or lactoferrin and C-reactive protein [ACG only]), and Giardia (in specific populations).16,57 The AGA also recommends considering bile acid diarrhea testing (48-hour fecal bile acid assay or serum fibroblast growth factor 19 level).57
A Diagnostic Algorithm for Chronic Diarrhea: Focusing on IBS-D and EPI
Utilizing the four-step procedure, we have refined and developed a straightforward algorithm to assist clinicians in differentiating IBS-D and EPI from other diarrhea syndromes (Fig. 3). This algorithm aims to minimize diagnostic testing and healthcare costs by avoiding unnecessary investigations, leading to more timely and appropriate diagnosis and management. The algorithm provides a simple framework for rapid and accurate IBS-D diagnosis. It starts with three “rule-in” questions aligned with Rome IV criteria for IBS: (1) Do you experience abdominal pain? (2) Does pain improve or worsen with defecation? (3) Is pain associated with changes in stool frequency or texture? Positive answers to these questions, in the absence of alarm symptoms/signs (Fig. 3), allow for IBS-D diagnosis with approximately 97% accuracy.13 In such cases, minimal diagnostic testing is needed. However, if alarm symptoms are present (e.g., weight loss) and EPI is suspected, nutritional markers and FE-1 testing are indicated. Abnormal results necessitate pancreatic investigation. If the pancreas appears normal, a false-positive FE-1 test is likely, EPI can be excluded, and other causes of chronic diarrhea should be explored.
DISCUSSION: Enhancing Diagnostic Accuracy in Chronic Diarrhea
Diarrhea is a prevalent and complex disorder arising from diverse etiologic and pathogenic mechanisms. Differentiating these conditions, especially with overlapping symptoms, can be challenging. This is particularly evident in IBS-D, where up to 75% of patients meeting diagnostic criteria in the United States remain undiagnosed.58 This is concerning as IBS is the most common cause of diarrhea and can be diagnosed accurately using simple binary questions and minimal testing.
Exocrine Pancreatic Insufficiency (EPI) is a significant mimic of IBS-D, often leading to misdiagnosis. Our proposed algorithm is specifically designed to aid in distinguishing between these two disorders (Fig. 3) and differentiating them from other causes of chronic diarrhea. Crucially, this algorithm incorporates recommendations from recent ACG and AGA IBS guidelines emphasizing a positive diagnostic strategy. This simplified algorithm should assist practitioners in achieving timely diagnoses and reducing unnecessary testing, thus minimizing treatment delays and improving patient health and quality of life.58
ACKNOWLEDGMENTS
The authors acknowledge Moira A. Hudson, PhD, and Janet E. Matsuura, PhD, of ICON plc for medical writing and editing support in manuscript development, funded by AbbVie.
Footnotes
AbbVie provided financial support for manuscript development and courtesy medical review; however, authors retained all content decisions. No honoraria or payments were made for authorship.
Disclosures:
D.M.B. consultant, advisor, or speaker for Alnylam, Alfasigma, Anji, Ardelyx, Arena, Bayer, AbbVie, Mahana, Owlstone, Ironwood, Salix, Takeda, Redhill, QoL Medical, Gemelli Biotech, and Vibrant; Board of Directors for IFFGD; unrestricted grants from IDP Foundation. J.E.D.-M. honoraria for lectures and advisory activities from AbbVie, Viatris, and Abbott Pharmaceuticals; unrestricted research grants from AbbVie.
Contributor Information
Darren M. Brenner, Email: [email protected].
J. Enrique Domínguez-Muñoz, Email: [email protected].