Down syndrome, also known as trisomy 21, is a genetic disorder arising from an extra copy of chromosome 21. This chromosomal anomaly leads to developmental changes affecting both the body and brain, resulting in intellectual disabilities and distinctive physical characteristics. Individuals with Down syndrome benefit significantly from early intervention and comprehensive support, enhancing their quality of life. As a lifelong condition, effective management and care planning are crucial, particularly from a nursing perspective.
What is Down Syndrome?
Down syndrome is primarily characterized by trisomy of chromosome 21, leading to a spectrum of systemic complications. It stands as the most frequently occurring chromosomal anomaly, affecting approximately 1 in 700 to 800 live births. First described by Langdon Down in 1866, the underlying cause remained unclear until 1959 when the chromosomal anomaly was identified. The syndrome’s effects are broad, impacting various aspects of health and development, necessitating a holistic approach to care.
Pathophysiology of Down Syndrome
The pathophysiology of Down syndrome is explained by two main hypotheses: developmental instability due to chromosomal imbalance, and the gene-dosage effect. The gene-dosage effect suggests that genes on chromosome 21 are overexpressed in individuals with Down syndrome, contributing to the observed phenotypic abnormalities. The Down Syndrome Critical Region (DSCR) on chromosome 21q22.1-q22.3 is particularly implicated in congenital heart diseases commonly seen in Down syndrome.
Physiologically, Down syndrome affects multiple systems. Thyroid metabolism and intestinal absorption are often abnormal, predisposing individuals to obesity. Impaired immune responses increase susceptibility to infections, and autoimmune conditions like hypothyroidism and Hashimoto thyroiditis are more prevalent. Patients also exhibit decreased physiological buffering, leading to hypersensitivity to certain medications and abnormal sensory responses. Metabolic processes are also affected, increasing the risk of hyperuricemia and insulin resistance. Furthermore, children with Down syndrome have a higher predisposition to leukemia, especially transient myeloproliferative disorder and acute megakaryocytic leukemia. Musculoskeletal issues include reduced stature, atlantooccipital and atlantoaxial hypermobility, and cervical vertebral malformations. Gastrointestinal manifestations, present in about 5% of cases, include duodenal atresia, Hirschsprung disease, and celiac disease.
Statistics and Incidence of Down Syndrome
Down syndrome is observed globally across all ethnicities. Approximately 6,000 children are born with Down syndrome each year. It is a significant contributor to intellectual disability, accounting for about one-third of moderate to severe cases in school-aged children. The prevalence of Down syndrome has increased worldwide due to increased lifespan of affected individuals. Morphological features become more evident as children age, typically after the first year. While generally sporadic, familial occurrences are rare, and recurrence risk is linked to maternal age. Newborn males are slightly more affected than females (ratio of approximately 1.15:1) in cases of free trisomy 21. Fertility in females with trisomy 21 is estimated at 50%, with each pregnancy having a 50% chance of resulting in a child with trisomy 21.
Causes of Down Syndrome
The exact cause of Down syndrome remains unknown, but several cytogenetic variants are identified:
- Full Trisomy 21: The most common type, resulting from nondisjunction during meiosis, where there are three full copies of chromosome 21. This is correlated with advanced maternal and paternal age.
- Translocation: A chromosomal translocation occurs when part of chromosome 21 attaches to another chromosome. Individuals have 46 chromosomes in total, but with extra material from chromosome 21.
- Mosaicism: This occurs post-fertilization and involves mitotic loss of a chromosome in a trisomic zygote. This results in two cell lines: one with trisomy 21 and another with a normal karyotype, leading to variable phenotypic expression.
Clinical Manifestations of Down Syndrome
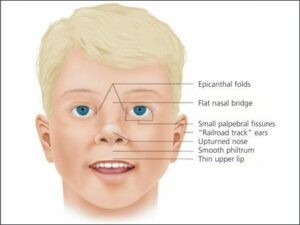
Characteristic craniofacial features are prominent in Down syndrome:
- Flattened facial appearance and occiput: Becomes noticeable by one year of age.
- Brachycephaly: Small and broad head shape.
- Epicanthal folds: Skin folds at the inner corner of the eyes.
- Flat nasal bridge: Short and flattened bridge of the nose.
- Upward-slanting palpebral fissures: Eyes appear almond-shaped and slant upwards.
- Brushfield spots: Speckling of the iris.
- Small nose and mouth: Proportionally smaller facial features.
- Protruding tongue: Often thick and fissured.
- Small and dysplastic ears.
- Generous nuchal skin: Excess skin at the nape of the neck.
Assessment and Diagnostic Findings for Down Syndrome
Diagnosis of Down syndrome typically begins with prenatal screening followed by definitive diagnostic testing.
- Laboratory Studies: Complete blood count (CBC) and bone marrow examination may be conducted to rule out leukemia. Thyroid function tests (TSH and T4) are crucial at birth, 6, 12 months, and annually to monitor for hypothyroidism. Papanicolaou smears are recommended every 1-3 years for sexually active women.
- Cytogenetic Studies: Karyotyping confirms trisomy 21 and is essential for genetic counseling, especially in translocation Down syndrome cases.
- Fluorescence in situ hybridization (FISH): FISH provides rapid diagnosis of trisomy 21, useful both prenatally and neonatally but needs karyotype confirmation to detect translocations.
- Prenatal Screening: Maternal serum biomarkers and ultrasonography can detect a high percentage of Down syndrome pregnancies.
- Nuchal Translucency (NT) Scan: Performed at 11-14 weeks, increased NT is associated with higher risk of Down syndrome and other genetic syndromes.
- Amniocentesis: Performed at 14-16 weeks, it is a highly accurate invasive diagnostic test for chromosomal disorders.
- Chorionic Villus Sampling (CVS): Performed at 10-13 weeks, it offers earlier diagnosis but carries a slight risk of fetal loss and limb deficiency.
Medical Management of Down Syndrome
Currently, there are no medical treatments to reverse the intellectual disability associated with Down syndrome. However, significant advancements in medical care have dramatically improved the quality of life and life expectancy.
- Surgical Care: Timely surgical intervention is crucial for cardiac anomalies detected in newborns or early infancy. Surgery might also be required for atlantoaxial subluxation and cervical spine stabilization if neurological deficits are present. Congenital cataracts, occurring in about 3% of children, require early surgical removal.
- Diet: No specific diet is needed unless celiac disease is diagnosed. A balanced diet and regular exercise are important for weight management. Feeding difficulties and failure to thrive may improve post-cardiac surgery.
- Activity: Physical activity is encouraged without restrictions, although caution is advised regarding sports with high spinal injury risks like football, soccer, and gymnastics. Exercise is recommended for maintaining a healthy weight.
- Pharmacologic Management: Standard immunizations and well-child care are essential. Specific manifestations and associated conditions are addressed pharmacologically as needed.
Nursing Management for Down Syndrome
Nursing management plays a vital role in the holistic care of individuals with Down syndrome, focusing on assessment, diagnosis, planning, intervention, and evaluation to optimize health outcomes and quality of life. A crucial aspect of nursing care is developing a robust Down Syndrome Nursing Diagnosis Care Plan.
Nursing Assessment for Down Syndrome
A comprehensive nursing assessment is the foundation of effective care. It includes:
- Physical Assessment: A thorough, systemic, head-to-toe assessment of the newborn and child. This involves detailed observation of physical characteristics associated with Down syndrome, including facial features, muscle tone, reflexes, and signs of any associated conditions like cardiac or respiratory issues.
- History: Gathering detailed history is crucial. This includes maternal pregnancy history, birth history, genetic testing results, developmental milestones, feeding patterns, growth patterns, and any medical history of the child and family.
Nursing Diagnoses for Down Syndrome
Based on the nursing assessment, common nursing diagnoses for individuals with Down syndrome may include:
- Risk for Aspiration related to hypotonia and feeding difficulties.
- Impaired Swallowing related to hypotonia and oral motor dysfunction.
- Imbalanced Nutrition: Less Than Body Requirements related to feeding difficulties and increased metabolic needs in some cases.
- Risk for Infection related to immune system dysfunction.
- Delayed Growth and Development related to genetic anomalies and developmental delays.
- Ineffective Airway Clearance related to hypotonia and potential respiratory complications.
- Risk for Injury related to hypotonia, developmental delays, and potential cardiac conditions.
- Deficient Knowledge (of caregivers) related to Down syndrome care and management.
- Compromised Family Coping related to the challenges of caring for a child with Down syndrome.
- Social Isolation related to developmental delays and societal barriers.
Nursing Care Planning and Goals for Down Syndrome
The nursing care plan for a child with Down syndrome is individualized and family-centered. Major goals are:
- Maintain a patent airway and prevent aspiration.
- Promote safe and effective feeding and adequate nutrition.
- Prevent infection and manage infections promptly.
- Optimize growth and development potential.
- Prevent injuries.
- Educate caregivers about Down syndrome and its management.
- Support family coping and adjustment.
- Facilitate social integration and participation.
Nursing Interventions for Down Syndrome
Nursing interventions are tailored to address the specific nursing diagnoses and achieve the established goals. Examples include:
- For Risk for Aspiration and Impaired Swallowing:
- Position infant upright during feeding.
- Provide small, frequent feedings.
- Use thickened liquids as prescribed.
- Teach parents safe feeding techniques and signs of aspiration.
- For Imbalanced Nutrition: Less Than Body Requirements:
- Monitor weight and growth regularly.
- Collaborate with dieticians for nutritional support.
- Encourage breastfeeding or formula feeding as appropriate.
- Address any underlying medical conditions affecting nutrition.
- For Risk for Infection:
- Maintain meticulous hygiene.
- Ensure timely immunizations.
- Educate caregivers on infection prevention and early signs of infection.
- For Delayed Growth and Development:
- Refer to early intervention programs and therapies (physical therapy, occupational therapy, speech therapy).
- Encourage developmental activities appropriate for the child’s age and abilities.
- Monitor developmental milestones and progress.
- For Ineffective Airway Clearance:
- Monitor respiratory status closely.
- Ensure proper positioning to promote lung expansion.
- Provide chest physiotherapy as needed.
- Educate caregivers on recognizing signs of respiratory distress.
- For Risk for Injury:
- Ensure a safe environment.
- Educate caregivers on safety precautions at home and in the community.
- Assess and address any cardiac conditions that increase injury risk.
- For Deficient Knowledge (of caregivers) and Compromised Family Coping:
- Provide comprehensive education about Down syndrome, its management, and available resources.
- Offer emotional support and counseling.
- Connect families with support groups and community resources.
- Encourage respite care and self-care for caregivers.
- For Social Isolation:
- Encourage participation in inclusive educational and recreational activities.
- Advocate for social inclusion and reduce stigma.
- Support families in accessing community support networks.
Evaluation of Nursing Care for Down Syndrome
Evaluation of nursing care is ongoing and focuses on whether the established goals are met. Goals are met as evidenced by:
- The child maintains a clear airway without aspiration.
- The child demonstrates safe and effective swallowing and achieves adequate nutritional intake.
- The child remains free from infection or infections are managed effectively.
- The child progresses in growth and development according to their potential.
- The child remains free from injury.
- Caregivers demonstrate adequate knowledge about Down syndrome and its management.
- Families demonstrate effective coping mechanisms and utilize available support systems.
- The child participates in social activities and experiences reduced isolation.
Documentation Guidelines for Down Syndrome
Accurate and comprehensive documentation is essential. Documentation should include:
- Detailed assessment findings.
- Nursing diagnoses identified.
- Individualized care plan.
- Nursing interventions implemented.
- Patient and family education provided.
- Evaluation of outcomes and progress toward goals.
- Availability and use of support systems and community resources.
- Deviations from normal parenting expectations and strategies to support parents.
By implementing a comprehensive Down syndrome nursing diagnosis care plan, nurses play a critical role in improving the health, development, and quality of life for individuals with Down syndrome and their families. This plan ensures that care is holistic, individualized, and responsive to the unique needs of each patient and family.