Nursing diagnosis is a cornerstone of effective patient care. As a clinical judgment, it pinpoints a patient’s response to health conditions or life processes, or their vulnerability to such responses. This guide will provide a comprehensive understanding of how to formulate nursing diagnoses, enhancing your ability to create targeted and effective nursing care plans.
Understanding Nursing Diagnosis
A nursing diagnosis serves as a clear statement of a patient’s health status, identifying issues that nurses are qualified and accountable to address. It is derived from a thorough nursing assessment, which is the initial phase of the nursing process. The diagnosis then directs the selection of nursing interventions aimed at achieving specific patient outcomes. Essentially, it’s the crucial link between assessment and planning in patient care.
The Purpose of Nursing Diagnosis
Nursing diagnoses are not merely labels; they serve several vital purposes:
- Enhancing Critical Thinking: For nursing students, formulating diagnoses hones problem-solving and critical thinking skills, essential for effective practice.
- Prioritizing Care: Diagnoses help nurses identify and prioritize patient needs, guiding the direction of nursing interventions based on urgency and importance.
- Quality Assurance and Accountability: They facilitate the formulation of measurable outcomes, crucial for meeting quality assurance standards and demonstrating the value of nursing care to payers.
- Understanding Patient Responses: Nursing diagnoses illuminate how individuals or groups respond to health challenges, considering their strengths and resources to address problems.
- Facilitating Communication: They establish a common language among nurses and the healthcare team, promoting clear and effective communication regarding patient needs and care strategies.
- Evaluating Care Effectiveness: Diagnoses provide a basis for evaluating the impact of nursing care, determining its benefits to the patient and its cost-effectiveness.
Nursing Diagnosis, Medical Diagnosis, and Collaborative Problems: Key Differences
It’s crucial to distinguish nursing diagnoses from medical diagnoses and collaborative problems.
A nursing diagnosis focuses on the patient’s response to a health condition. For instance, a patient with pneumonia might have the nursing diagnosis “Ineffective Airway Clearance related to excessive mucus production.” This diagnosis directs nursing care towards managing secretions and improving breathing.
Medical diagnoses, on the other hand, are made by physicians and identify diseases or pathological states that physicians treat. Examples include Pneumonia, Diabetes Mellitus, or Heart Failure. Medical diagnoses focus on the disease process itself.
Collaborative problems are potential or actual health complications that require both medical and nursing interventions. Nurses manage these by monitoring patient conditions and implementing physician-prescribed treatments alongside independent nursing actions. For example, managing the potential complication of respiratory distress in a patient with pneumonia is a collaborative problem.
In essence, nursing diagnoses address patient responses to health issues, medical diagnoses name diseases, and collaborative problems involve managing complications requiring interdisciplinary care.
Classification: Organizing Nursing Diagnoses with Taxonomy II
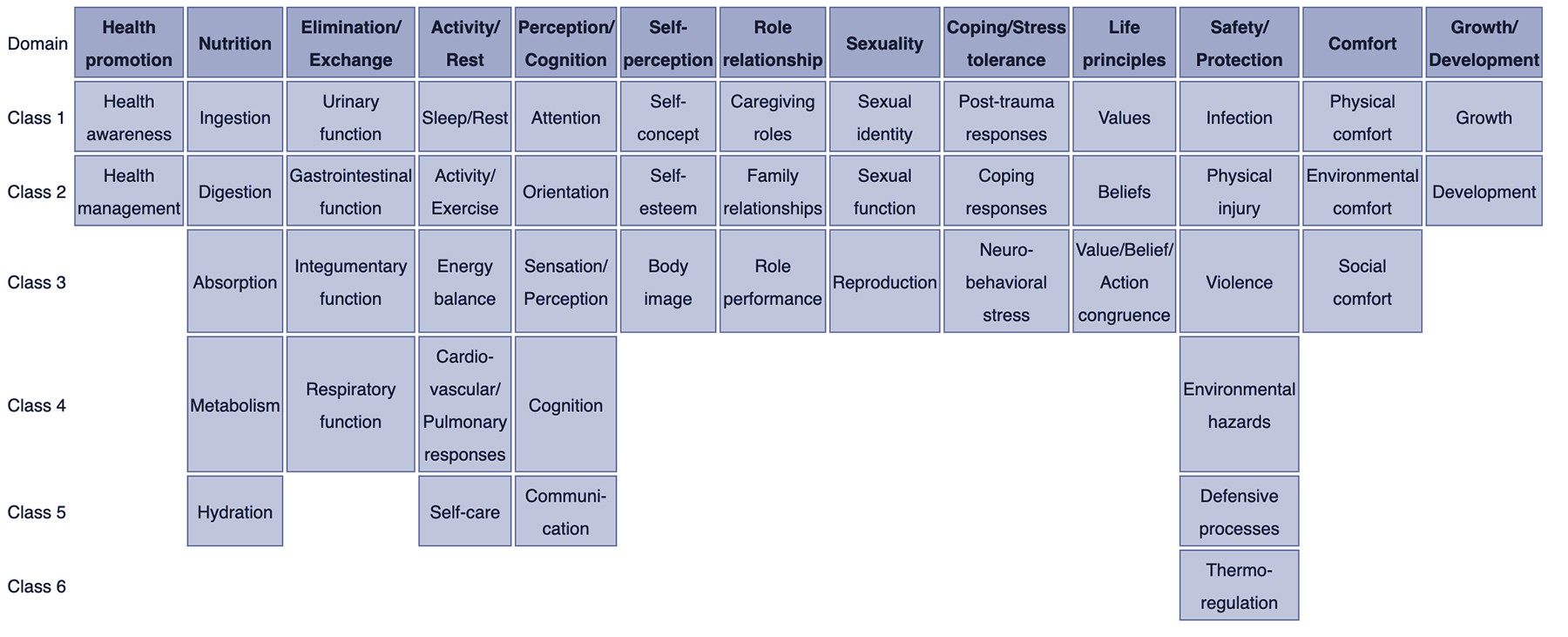
To standardize and organize nursing diagnoses, Taxonomy II was adopted in 2002. This system, based on Dr. Mary Joy Gordon’s Functional Health Patterns, arranges diagnoses into a hierarchical structure:
- Domains (13): Broad areas of health, such as Health Promotion, Nutrition, Activity/Rest, and Safety/Protection.
- Classes (47): Subcategories within domains, like Health Awareness, Ingestion, Sleep/Rest, and Infection.
- Nursing Diagnoses: Specific diagnostic labels within classes, listed alphabetically by concept.
Taxonomy II uses a multi-axial system for coding diagnoses, considering: diagnostic concept, time, unit of care, age, health status, descriptor, and topology. This classification provides a structured framework for nurses to select appropriate and standardized diagnoses.
Nursing Diagnosis within the Nursing Process
Nursing diagnosis is the second crucial step in the nursing process, following assessment and preceding planning, implementation, and evaluation. The nursing process is a systematic, patient-centered approach to care.
- Assessment: Gathering comprehensive patient data (subjective and objective).
- Diagnosis: Analyzing assessment data to identify patient problems and needs – this is where nursing diagnosis formulation occurs.
- Planning: Developing a care plan with specific goals and interventions based on the nursing diagnoses.
- Implementation: Carrying out the nursing interventions outlined in the care plan.
- Evaluation: Assessing the effectiveness of interventions and patient progress towards goals.
Each stage of the nursing process relies on critical thinking. A strong understanding of nursing diagnoses is essential for nurses to identify patient needs, select appropriate interventions, and ultimately, provide effective care.
Types of Nursing Diagnoses
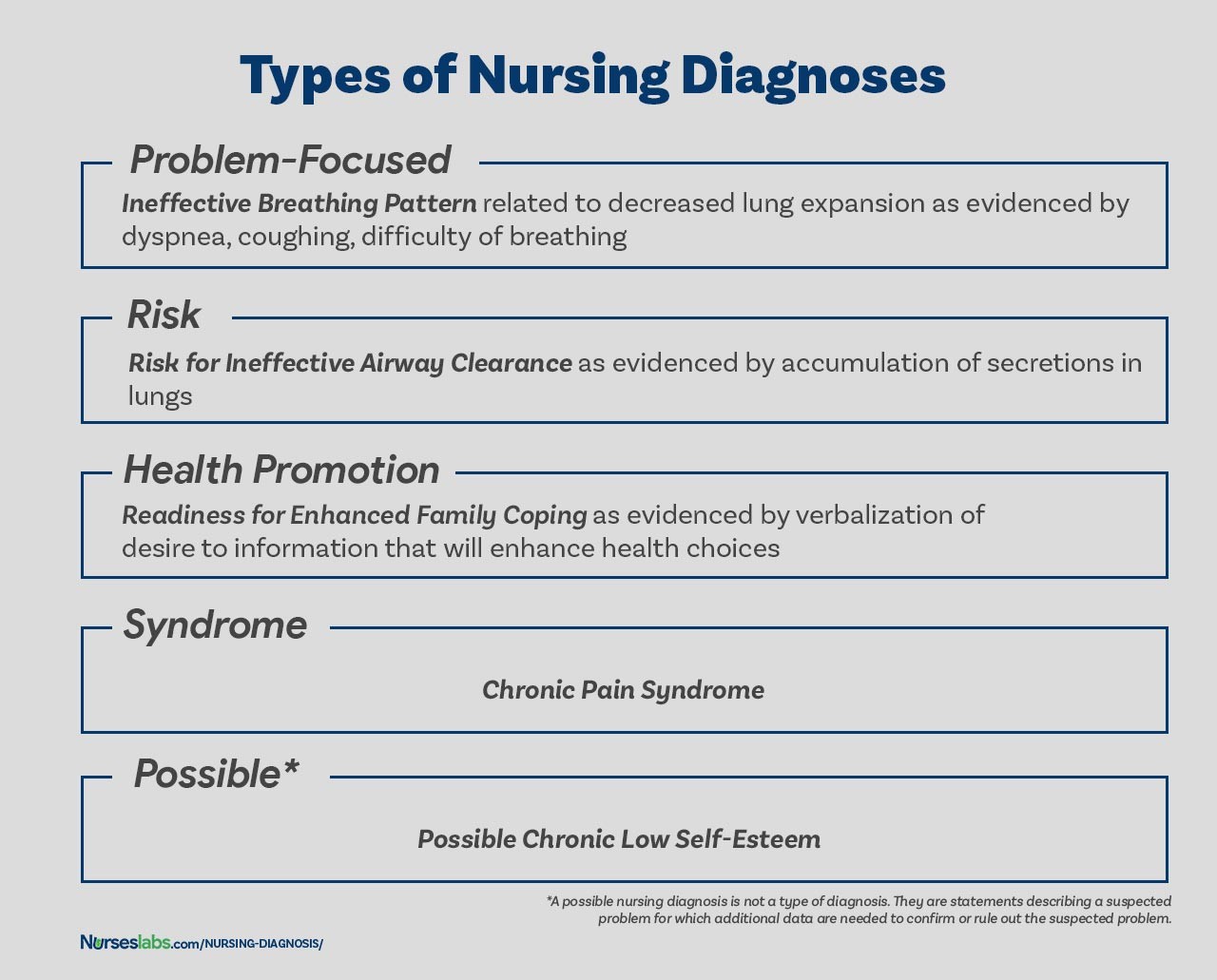
Nursing diagnoses are categorized into four main types, each serving a distinct purpose in patient care:
1. Problem-Focused (Actual) Nursing Diagnosis
A problem-focused diagnosis, also known as an actual diagnosis, describes a current problem that the patient is experiencing at the time of assessment. It is supported by defining characteristics – the signs and symptoms that indicate the presence of the problem.
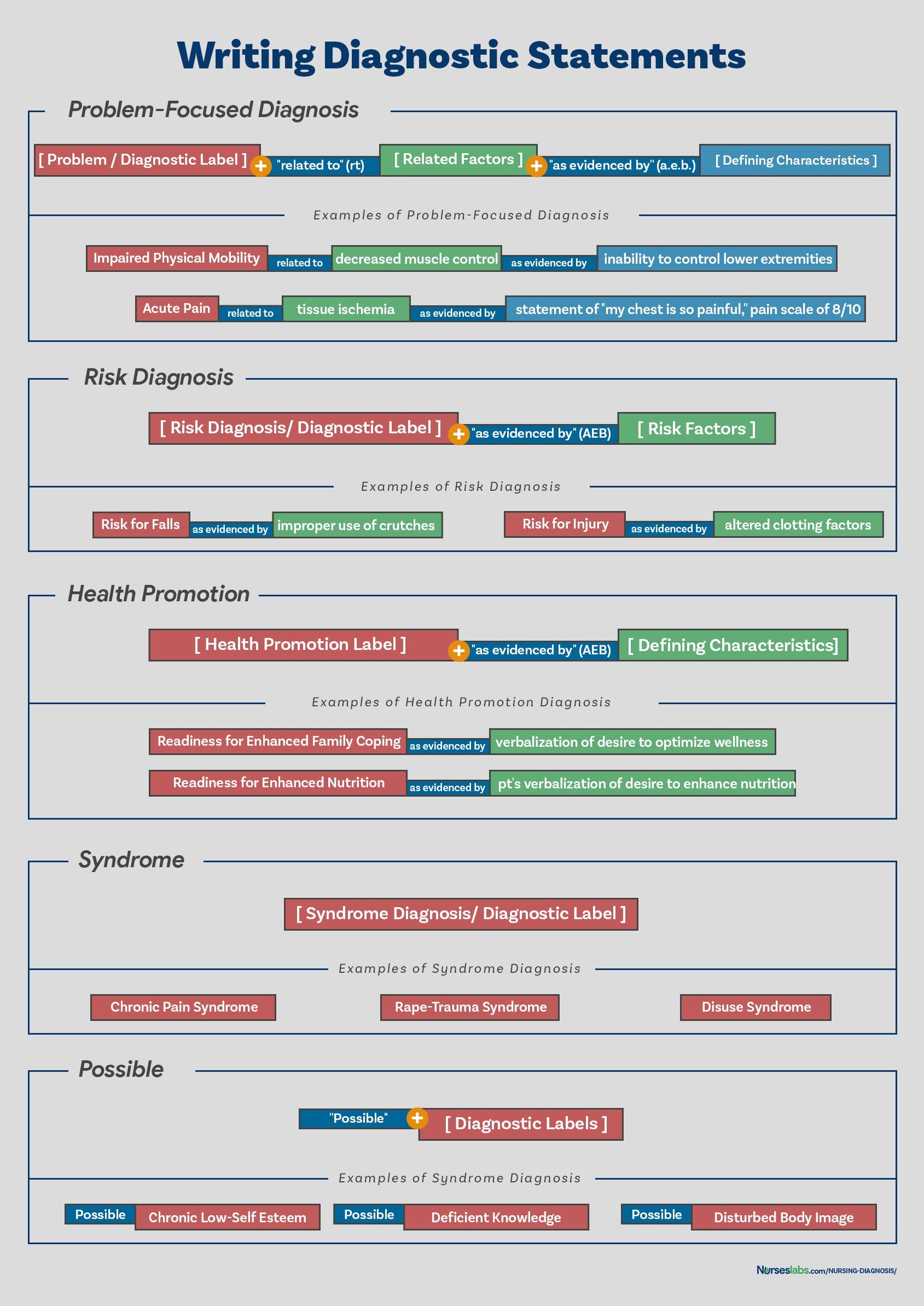
These diagnoses have three components:
- Nursing Diagnosis Label: A concise term describing the problem (e.g., “Acute Pain”).
- Related Factors: The underlying cause or contributing factors to the problem (e.g., “related to surgical incision”).
- Defining Characteristics: The observable signs and symptoms (e.g., “as evidenced by patient reporting pain level of 7/10, guarding behavior, and increased heart rate”).
Example: Acute Pain related to surgical incision as evidenced by patient reporting pain level of 7/10, guarding behavior, and increased heart rate.
2. Risk Nursing Diagnosis
A risk nursing diagnosis identifies potential problems that a patient is vulnerable to developing. It indicates that risk factors are present that increase the patient’s susceptibility to a problem, even if the problem doesn’t currently exist. These diagnoses are crucial for preventive care.
Risk diagnoses have two components:
- Risk Diagnosis Label: Describes the potential problem (e.g., “Risk for Infection”).
- Risk Factors: Factors that increase the patient’s vulnerability (e.g., “as evidenced by surgical wound, compromised immune system, and prolonged hospitalization”).
Example: Risk for Infection as evidenced by surgical wound, compromised immune system, and prolonged hospitalization.
It’s important to note that risk diagnoses do not include defining characteristics because the problem has not yet developed. Instead, “as evidenced by” connects the diagnosis label to the risk factors.
3. Health Promotion Nursing Diagnosis
A health promotion diagnosis focuses on a patient’s desire and motivation to improve their well-being and health. It identifies a patient’s readiness to enhance specific health behaviors.
These diagnoses typically have one component:
- Nursing Diagnosis Label: Describes the area for health enhancement (e.g., “Readiness for Enhanced Nutrition”).
Example: Readiness for Enhanced Nutrition.
Related factors, such as “expressed interest in learning about healthy eating,” can be added to provide further clarity, but are not always required.
4. Syndrome Nursing Diagnosis
A syndrome diagnosis is used when a cluster of nursing diagnoses frequently occur together due to a specific event or situation. It recognizes a predictable pattern of diagnoses.
Syndrome diagnoses have one component:
- Syndrome Diagnosis Label: Identifies the cluster of diagnoses (e.g., “Rape-Trauma Syndrome”).
Example: Rape-Trauma Syndrome.
5. Possible Nursing Diagnosis (Not a Type, but a Category of Statement)
A possible nursing diagnosis describes a suspected problem that requires further data collection to confirm or rule out. It’s not a formal type of diagnosis like the previous four, but rather a category of diagnostic statement used when more information is needed.
Example: Possible Ineffective Coping related to unclear stressors. (Further assessment is needed to identify the stressors and confirm Ineffective Coping).
Components of a Nursing Diagnosis Statement
A well-formulated nursing diagnosis typically includes three key components, especially for problem-focused diagnoses:
- Problem (Diagnostic Label): A concise statement of the patient’s health problem.
- Etiology (Related Factors): The cause or contributing factors to the problem.
- Defining Characteristics (Signs and Symptoms): Evidence that the problem exists.
For risk diagnoses, etiology is replaced by risk factors. Health promotion and syndrome diagnoses often use a one-part statement (diagnostic label only).
1. Problem and Definition (Diagnostic Label)
The problem statement, or diagnostic label, is a standardized term that concisely describes the patient’s health response. It usually consists of two parts:
- Qualifier (Modifier): Words that add specific meaning or detail to the diagnosis.
- Focus of the Diagnosis: The area of health concern.
| Qualifier | Focus of the Diagnosis |
|---|---|
| Deficient | Fluid Volume |
| Imbalanced | Nutrition: Less Than Body Requirements |
| Impaired | Gas Exchange |
| Ineffective | Tissue Perfusion |
| Risk for | Injury |
Some diagnoses are single words (e.g., Anxiety, Constipation), where the qualifier and focus are inherent in the term.
2. Etiology (Related Factors)
The etiology, or related factors, identifies the probable causes or contributing factors to the nursing diagnosis. It’s crucial because interventions should be directed at addressing these underlying causes. Etiology is linked to the problem statement using the phrase “related to.”
Example: Impaired Physical Mobility related to pain and stiffness. (Pain and stiffness are the etiological factors contributing to impaired mobility).
3. Risk Factors (For Risk Diagnoses)
For risk nursing diagnoses, risk factors replace etiological factors. Risk factors are circumstances or conditions that increase a patient’s vulnerability to a problem. They are also linked to the diagnosis label using “as evidenced by.”
Example: Risk for Falls as evidenced by muscle weakness and history of falls. (Muscle weakness and fall history are risk factors for falls).
4. Defining Characteristics (Signs and Symptoms)
Defining characteristics are the observable cues (signs and symptoms) that cluster together and indicate the presence of an actual nursing diagnosis. They provide evidence for the diagnosis and are linked to the problem statement using “as evidenced by” or “as manifested by.”
Example: Ineffective Breathing Pattern related to pain as evidenced by shortness of breath, use of accessory muscles, and altered chest excursion. (Shortness of breath, accessory muscle use, and altered chest excursion are defining characteristics of Ineffective Breathing Pattern).
The Diagnostic Process: Step-by-Step
Formulating accurate nursing diagnoses involves a systematic three-phase process:
- Data Analysis: Examining the collected assessment data.
- Identification of Health Problems, Risks, and Strengths: Interpreting data to pinpoint specific issues.
- Formulation of Diagnostic Statements: Writing clear and concise nursing diagnoses.
Phase 1: Analyzing Data
Data analysis involves several key steps:
- Comparing Data to Standards: Comparing patient data to established norms and healthy ranges to identify deviations.
- Clustering Cues: Grouping related data cues together to identify patterns and potential problems.
- Identifying Gaps and Inconsistencies: Recognizing missing information or conflicting data that requires further investigation.
Phase 2: Identifying Health Problems, Risks, and Strengths
In this phase, nurses use critical thinking to interpret the analyzed data and determine:
- Nursing Diagnoses: Identifying actual or potential health problems that fall within the scope of nursing practice.
- Medical Diagnoses: Recognizing conditions that require medical diagnosis and treatment.
- Collaborative Problems: Identifying situations requiring both medical and nursing interventions.
- Patient Strengths: Recognizing patient resources, coping mechanisms, and areas of wellness that can be leveraged in the care plan.
This step involves prioritizing identified problems based on urgency and patient needs.
Phase 3: Formulating Diagnostic Statements
This final phase involves constructing the actual written nursing diagnosis statements. The format depends on the type of diagnosis (problem-focused, risk, health promotion, or syndrome). The goal is to create statements that are:
- Clear and Concise: Easy to understand and interpret.
- Specific: Accurately reflect the patient’s health status.
- Accurate: Supported by assessment data.
- Related to Etiology/Risk Factors: Identify contributing factors to guide interventions.
How to Write a Nursing Diagnosis: Statement Formats
The way you write a nursing diagnosis statement depends on the type of diagnosis. Different formats ensure clarity and completeness.
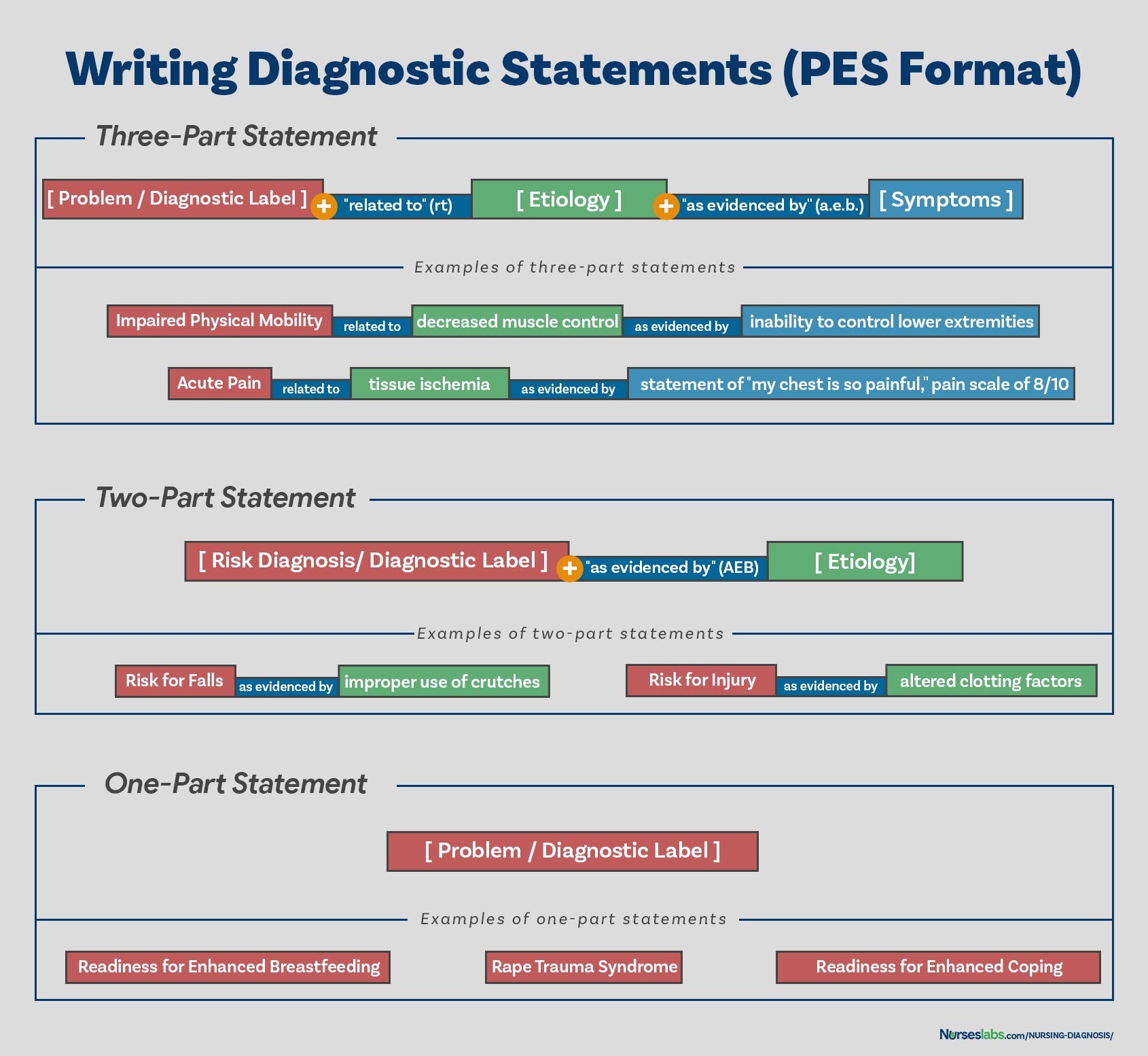
Using the PES Format
The PES format is a common and helpful structure for writing nursing diagnoses, particularly for problem-focused diagnoses. PES stands for:
- Problem (Diagnostic Label)
- Etiology (Related Factors)
- Signs/Symptoms (Defining Characteristics)
Nursing diagnosis statements can be one-part, two-part, or three-part, often utilizing the PES format components as appropriate for the diagnosis type.
One-Part Nursing Diagnosis Statements
Health promotion diagnoses and syndrome diagnoses are typically written as one-part statements, including only the diagnostic label.
- Health Promotion Diagnosis Example: Readiness for Enhanced Coping
- Syndrome Diagnosis Example: Rape-Trauma Syndrome
For health promotion diagnoses, the related factor is often implied (“motivated to enhance wellness”). Syndrome diagnoses, by definition, are clusters of problems with a common etiology, so related factors are inherent in the syndrome itself.
Two-Part Nursing Diagnosis Statements
Risk diagnoses and possible diagnoses are generally written as two-part statements.
-
Risk Diagnosis: Diagnostic label linked to risk factors using “as evidenced by.”
- Example: Risk for Infection as evidenced by weakened immune system response.
-
Possible Diagnosis: Diagnostic label linked to the reason for suspicion using “related to.”
- Example: Possible Ineffective Coping related to unclear stressors.
Two-part statements for risk and possible diagnoses do not include signs and symptoms because the problem is either potential or suspected, not yet confirmed by defining characteristics.
Three-Part Nursing Diagnosis Statements
Problem-focused (actual) diagnoses are best written as three-part statements, utilizing the full PES format:
- Problem (P): Diagnostic label.
- Etiology (E): Related factors, linked with “related to.”
- Signs/Symptoms (S): Defining characteristics, linked with “as evidenced by.”
Example: Ineffective Airway Clearance related to excessive mucus production as evidenced by cough, coarse crackles on auscultation, and shortness of breath.
This three-part statement clearly identifies the problem, its cause, and the supporting evidence, providing a comprehensive and actionable nursing diagnosis.
Nursing Diagnosis for Care Plans
Nursing diagnoses are the foundation of nursing care plans. They directly guide the development of patient-centered goals and nursing interventions. By accurately identifying patient problems and their underlying causes, nurses can create targeted care plans to address specific needs and promote positive patient outcomes.
For an extensive list of nursing diagnosis examples that can be used in care plans, refer to resources like “Nursing Care Plans (NCP): Ultimate Guide and List.”
Recommended Resources for Deeper Learning
To further enhance your understanding and skills in formulating nursing diagnoses, consider these recommended resources:
-
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care: A comprehensive handbook with an evidence-based approach to nursing interventions, guiding you through assessment, diagnosis, and care planning.
-
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition): Features over 200 care plans reflecting current evidence-based guidelines, including ICNP diagnoses and expanded content on various health topics.
-
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales: A quick-reference tool for identifying correct diagnoses and planning care efficiently, updated with the latest diagnoses and interventions.
-
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care: Provides interventions for over 800 diseases and disorders, with detailed information for each diagnosis, including clinical applications and documentation guidance.
-
All-in-One Nursing Care Planning Resource – E-Book: Medical-Surgical, Pediatric, Maternity, and Psychiatric-Mental Health: Includes over 100 care plans across various specialties, focusing on interprofessional “patient problems.”
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition)
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care
Conclusion
Mastering the formulation of nursing diagnoses is a fundamental skill for every nurse. By understanding the types of diagnoses, their components, and the diagnostic process, you can accurately identify patient needs and create effective care plans. This guide has provided a step-by-step approach to formulating nursing diagnoses, empowering you to enhance your clinical judgment and contribute to improved patient care. Consistent practice and utilization of available resources will solidify your expertise in this critical area of nursing practice.
References and Sources
- Berman, A., Snyder, S., & Frandsen, G. (2016). Kozier & Erb’s Fundamentals of Nursing: Concepts, process and practice. Boston, MA: Pearson.
- Edel, M. (1982). The nature of nursing diagnosis. In J. Carlson, C. Craft, & A. McGuire (Eds.), Nursing diagnosis (pp. 3-17). Philadelphia: Saunders.
- Fry, V. (1953). The Creative approach to nursing. AJN, 53(3), 301-302.
- Gordon, M. (1982). Nursing diagnosis: Process and application. New York: McGraw-Hill.
- Gordon, M. (2014). Manual of nursing diagnosis. Jones & Bartlett Publishers.
- Gebbie, K., & Lavin, M. (1975.) Classification of nursing diagnoses: Proceedings of the First National Conference. St. Louis, MO: Mosby.
- McManus, R. L. (1951). Assumption of functions in nursing. In Teachers College, Columbia University, Regional planning for nurses and nursing education. New York: Columbia University Press.
- Powers, P. (2002). A discourse analysis of nursing diagnosis. Qualitative health research, 12(7), 945-965.