Table of Contents
What is a Nursing Care Plan?
A nursing care plan (NCP) is a structured, dynamic, and patient-centered guide used by nurses to deliver holistic and effective care. It is a formal process that meticulously identifies a patient’s current health needs, potential risks, and outlines strategies to address them. Crucially, the nursing care plan incorporates nursing diagnoses, which are clinical judgments about individual, family, or community experiences/responses to actual or potential health problems/life processes. These diagnoses form the foundation upon which the entire care plan is built.
Nursing care plans serve as a vital communication tool among nurses, patients, and the interdisciplinary healthcare team. They ensure everyone is aligned on the patient’s needs, goals, and the plan of action. Without a well-defined nursing care planning process, the consistency and quality of patient care can be significantly compromised. The integration of nursing diagnosis into the care plan ensures that interventions are targeted and directly address the patient’s specific health issues and responses.
The process of nursing care planning begins at the point of patient admission and is a living document, continuously updated to reflect changes in the patient’s condition, new nursing diagnoses, and the evaluation of goal achievement. This dynamic approach to care planning, centered around accurate nursing diagnoses, is fundamental to delivering individualized and patient-centered care, which is the cornerstone of excellence in nursing practice.
Types of Nursing Care Plans
Nursing care plans can be broadly categorized as informal or formal, each serving different purposes in patient care management:
- Informal Nursing Care Plans: These are mental strategies or action plans that a nurse develops in their mind. They are not written down and are typically used for routine care or in situations where quick adjustments are needed.
- Formal Nursing Care Plans: These are documented guides, either written or computerized, that systematically organize a patient’s care information. Formal care plans are essential for comprehensive care, communication, and continuity across different shifts and healthcare providers.
Formal nursing care plans are further divided into standardized and individualized care plans, offering different levels of specificity and customization:
- Standardized Care Plans: These are pre-written care plans that outline nursing care for patients with common needs or medical conditions. They are designed to ensure consistent care for groups of patients with similar diagnoses and to streamline nursing practice.
- Individualized Care Plans: These are tailored care plans developed to meet the unique needs of a specific patient. They are created by adapting standardized care plans or developing entirely new plans to address needs not covered in standardized formats, often arising from specific nursing diagnoses unique to the patient.
Standardized Care Plans
Standardized care plans are essential tools in healthcare settings, providing pre-approved guidelines developed by nursing staff and healthcare agencies. Their primary purpose is to guarantee that patients with specific conditions receive a consistent and baseline level of care. By outlining common interventions and expected outcomes for particular conditions, standardized care plans ensure that essential criteria are met for all patients. These plans are particularly valuable in promoting efficient use of nursing time by eliminating the need to repeatedly develop care strategies for frequently encountered patient needs.
It’s important to recognize that while standardized care plans offer a solid foundation, they are not designed to address the nuances of each patient’s unique situation. They should be viewed as a starting point, a template that needs to be further developed into an individualized care plan that incorporates specific nursing diagnoses and patient goals.
The care plans listed in this guide are examples of standard care plans. They are intended to serve as a framework or direction for nurses to develop individualized care plans that are precisely tailored to each patient’s needs and circumstances.
Individualized Care Plans
An individualized care plan represents the pinnacle of patient-centered care. It involves a deliberate process of modifying a standardized care plan or creating a new one from scratch to precisely align with the unique needs, preferences, and goals of an individual patient. This approach emphasizes using interventions and strategies that are proven to be effective for that particular patient, considering their specific nursing diagnoses. Individualized care plans acknowledge that each patient is unique and that their care should reflect this individuality. This holistic approach considers not just the disease or condition but also the patient’s strengths, resources, and personal goals.
Furthermore, individualized care plans have been shown to significantly improve patient satisfaction. When patients perceive that their care is specifically designed for them and responsive to their individual needs, they are more likely to feel valued, understood, and respected. This enhanced sense of patient engagement and personalized attention leads to greater satisfaction with their overall healthcare experience. In today’s healthcare landscape, where patient satisfaction is increasingly recognized as a critical indicator of quality care, the role of individualized care plans and accurate nursing diagnoses becomes even more paramount.
Tips on how to individualize a nursing care plan:
- Thorough Assessment: Begin with a comprehensive patient assessment to identify specific needs, preferences, and goals. This assessment is crucial for formulating accurate and relevant nursing diagnoses.
- Patient Involvement: Actively involve the patient and their family in the care planning process. Their input is invaluable in understanding their priorities and tailoring the plan to their lifestyle and values.
- Flexible Goals: Set goals that are realistic and achievable for the individual patient, taking into account their current health status, resources, and support system.
- Customized Interventions: Select nursing interventions that are specifically suited to the patient’s nursing diagnoses and unique needs. Consider their preferences, cultural background, and past experiences.
- Regular Review: Continuously evaluate and revise the care plan in response to changes in the patient’s condition, progress towards goals, and any new nursing diagnoses that emerge.
Objectives
The objectives of writing a nursing care plan are multifaceted and aim to improve the quality and effectiveness of patient care:
- Promote Evidence-Based Nursing Care: Nursing care plans are designed to incorporate the latest research and best practices in nursing. By using evidence-based interventions, care plans ensure that patients receive the most effective and up-to-date care. This includes using nursing diagnoses that are recognized and validated within the nursing profession.
- Support Holistic Care: A core objective of nursing care planning is to address the patient as a whole person. This means considering their physical, psychological, social, and spiritual needs. Nursing diagnoses help to identify issues in each of these dimensions, allowing for comprehensive care.
- Establish Care Pathways and Bundles: Care plans facilitate the development of structured care pathways and care bundles. Care pathways are collaborative, team-based approaches to standardize care and expected outcomes for specific patient groups. Care bundles are sets of evidence-based practices for specific conditions, ensuring consistent and optimal care delivery.
- Identify and Distinguish Goals and Expected Outcomes: Care plans clearly define patient goals and expected outcomes. Goals are broad statements of desired change, while expected outcomes are specific, measurable criteria to evaluate goal achievement. This clarity is essential for effective care management and evaluation, and directly linked to addressing the identified nursing diagnoses.
- Enhance Communication and Documentation: Nursing care plans improve communication among healthcare providers by providing a centralized, documented plan of care. They also serve as a formal record of the care provided, including nursing diagnoses, interventions, and patient responses.
- Measure Nursing Care Effectiveness: By outlining expected outcomes and providing a framework for evaluation, nursing care plans enable nurses to measure the effectiveness of their interventions and the overall quality of care provided. The achievement of outcomes directly relates to the appropriateness and accuracy of the initial nursing diagnoses.
Purposes of a Nursing Care Plan
Nursing care plans serve several critical purposes that contribute to improved patient care and professional nursing practice:
- Defines Nurse’s Role: Care plans highlight the unique and independent role of nurses in patient care. They emphasize the nurse’s responsibility in addressing patients’ overall health and well-being, going beyond simply following physician’s orders. Formulating nursing diagnoses is a key aspect of this independent role.
- Provides Direction for Individualized Care of the Client: A care plan acts as a roadmap for patient care. It guides nurses in critically thinking about each patient’s unique needs and developing tailored interventions. The nursing diagnosis is the starting point for this individualized approach.
- Ensures Continuity of Care: Care plans facilitate consistent care delivery across different nursing shifts and departments. By providing a shared source of information, they ensure that all nurses involved in a patient’s care are aware of the plan and can provide consistent interventions, leading to better patient outcomes.
- Coordinates Care: Care plans promote interdisciplinary collaboration by ensuring all members of the healthcare team are informed about the patient’s needs and the planned actions. This coordination prevents gaps in care and ensures a cohesive approach to patient management.
- Documentation: Care plans serve as formal documentation of the nursing process. They outline observations, nursing actions, and patient education needs. Accurate documentation in the care plan is critical for demonstrating the care provided and for legal and reimbursement purposes. The nursing diagnosis is a crucial element of this documentation.
- Guides Staff Assignment: In situations where patients require specialized care, care plans can inform staff assignments. They help ensure that patients are assigned to nurses with the appropriate skills and expertise to meet their specific needs.
- Monitors Progress: Care plans enable nurses to track patient progress towards goals and make necessary adjustments to the plan as needed. Regular evaluation and revision of the care plan, based on patient responses and evolving nursing diagnoses, is essential.
- Supports Reimbursement: Care plans, as part of the medical record, provide essential documentation for insurance companies. They justify the medical necessity and complexity of care provided, influencing reimbursement for healthcare services.
- Defines Client’s Goals: By involving patients in the development of their care plans, nurses empower patients and promote shared decision-making. This collaborative approach ensures that care is aligned with patient values and preferences, enhancing patient engagement and adherence to the plan. Patient goals are directly linked to addressing their nursing diagnoses.
Components
A comprehensive nursing care plan (NCP) typically includes several key components that work together to guide patient care. These components are:
- Nursing Diagnoses: These are clinical judgments about the patient’s responses to actual or potential health problems. They provide the basis for selecting nursing interventions to achieve outcomes for which the nurse is accountable. Nursing diagnoses are the foundation of the care plan.
- Client Problems: This section may describe patient problems in broader terms, often derived from the medical diagnosis or patient presentation. These problems are then refined into specific nursing diagnoses.
- Expected Outcomes: These are specific, measurable, achievable, relevant, and time-bound (SMART) statements that describe the desired changes in patient health status as a result of nursing care. Outcomes are directly linked to resolving the nursing diagnoses.
- Nursing Interventions: These are the specific actions that nurses will perform to achieve the expected outcomes. Interventions should be evidence-based and tailored to address the identified nursing diagnoses.
- Rationales: These are the scientific principles or evidence that support the chosen nursing interventions. Rationales explain why a particular intervention is expected to be effective in achieving the desired outcome and resolving the nursing diagnosis.
- Evaluation: This component describes how the nurse will evaluate the patient’s progress towards achieving the expected outcomes. Evaluation is an ongoing process that helps determine the effectiveness of the care plan and the need for revisions based on the patient’s response to interventions and changes in nursing diagnoses.
These components are interconnected and work in a cyclical process. The nursing diagnosis drives the selection of outcomes and interventions, and evaluation informs whether the plan is effective and if adjustments are needed.
Care Plan Formats
Nursing care plans can be organized in various formats, often using columns to structure the information clearly. Common formats include three-column, four-column, and five-column plans, each with slight variations in how the components are arranged. The core elements of nursing diagnoses, desired outcomes, interventions, and evaluation are consistent across formats.
Three-Column Format
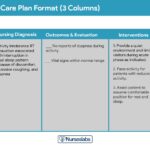
The three-column format is a simplified approach that combines related elements into single columns. Typically, it includes:
- Nursing Diagnosis: This column lists the identified nursing diagnoses.
- Outcomes and Evaluation: This column combines the desired patient outcomes and the criteria for evaluating whether those outcomes have been met.
- Interventions: This column outlines the specific nursing interventions planned to address the nursing diagnoses and achieve the desired outcomes.
Three-column nursing care plan format
Four-Column Format
The four-column format provides a more detailed structure by separating outcomes and evaluation into distinct columns. It typically includes:
- Nursing Diagnosis: Lists the identified nursing diagnoses.
- Goals and Outcomes: Specifies the desired patient goals and the measurable outcomes expected.
- Interventions: Outlines the nursing interventions to be implemented.
- Evaluation: Details how the patient’s progress will be evaluated in relation to the outcomes and nursing diagnoses.
Four-column nursing care plan template
Below is a document containing sample templates for the different nursing care plan formats. These templates are designed to help nurses organize and document patient care effectively, ensuring that nursing diagnoses, outcomes, interventions, and evaluation are clearly articulated.
Download: Printable Nursing Care Plan Templates and Formats
Student Care Plans
Student care plans are designed to be more in-depth and comprehensive than those used by practicing nurses. This is because they serve as a crucial learning tool for nursing students, helping them develop critical thinking, clinical reasoning, and care planning skills. Student care plans place a strong emphasis on the rationale behind each intervention and the link between nursing diagnoses and care strategies.
Student nursing care plans are more detailed.
Often, student care plans are required to be handwritten to reinforce the learning process and encourage thoroughness. A key difference in student care plans is the inclusion of an additional column for “Rationale” or “Scientific Explanation.” This column follows the nursing interventions column and requires students to articulate the scientific principles that justify the selection of each nursing intervention and its relevance to the nursing diagnosis. This emphasis on rationale helps students connect theoretical knowledge with practical application in patient care.
Writing a Nursing Care Plan
Developing an effective nursing care plan involves a systematic approach, following a series of steps within the nursing process. The process begins with a thorough assessment to identify nursing diagnoses, and progresses through planning, implementation, and evaluation.
Step 1: Data Collection or Assessment
The initial step in crafting a nursing care plan is comprehensive data collection, forming the foundation for accurate nursing diagnoses. This involves creating a detailed patient database using various assessment techniques and data collection methods. These methods include:
- Physical Assessment: A hands-on examination of the patient’s body systems to identify physical health issues.
- Health History: Gathering information about the patient’s past and present health status, including medical conditions, surgeries, medications, allergies, and lifestyle factors.
- Interview: Directly communicating with the patient (and family, when appropriate) to gather subjective data about their symptoms, concerns, and perceptions of their health.
- Medical Records Review: Examining the patient’s existing medical records, including physician’s notes, lab results, and previous treatment history.
- Diagnostic Studies: Reviewing results from laboratory tests, imaging studies, and other diagnostic procedures.
A comprehensive patient database encompasses all the health information collected through these methods. During this stage, nurses use their clinical judgment to identify patterns, significant findings, and potential health problems. This analysis helps in recognizing related or risk factors and defining characteristics that will be used to formulate specific nursing diagnoses. Many healthcare agencies and nursing schools provide specific assessment formats to guide this data collection process and ensure consistency and thoroughness.
Critical thinking is paramount during patient assessment. It requires integrating knowledge from various scientific disciplines and professional guidelines to inform clinical evaluations. This cognitive process, crucial for complex clinical decision-making, aims to effectively identify patients’ healthcare needs, leveraging a supportive environment and reliable information to arrive at accurate nursing diagnoses.
Step 2: Data Analysis and Organization
Once comprehensive patient data is collected, the next step is data analysis and organization. This involves a careful review of the gathered information to identify significant patterns, trends, and potential health problems. The process includes:
- Analyzing Data: Examining the collected data to differentiate between normal and abnormal findings, identify health problems, and recognize patient strengths.
- Clustering Data: Grouping related cues or data together to identify patterns that suggest specific health issues. This clustering helps in identifying potential nursing diagnoses.
- Organizing Data: Structuring the data in a logical manner, often using frameworks like body systems or Gordon’s Functional Health Patterns, to facilitate the identification of nursing diagnoses and prioritize patient needs.
This step is crucial for moving from raw data to actionable nursing diagnoses, priorities, and desired outcomes that will guide the rest of the care planning process.
Step 3: Formulating Your Nursing Diagnoses
Nursing diagnoses are the core of the nursing care plan. They are standardized, concise statements that describe a patient’s health problems or potential problems that nurses are qualified and licensed to treat. Nursing diagnoses differ from medical diagnoses, which identify diseases; instead, nursing diagnoses focus on the patient’s responses to health conditions and life processes.
Formulating accurate nursing diagnoses is essential for effective care planning. It involves:
- Identifying Problem: Recognizing the patient’s health issue based on the analyzed data.
- Writing Diagnostic Statement: Constructing a standardized nursing diagnosis statement using a recognized classification system, such as NANDA-I. A typical format includes:
- Problem: A concise label for the patient’s health issue.
- Etiology (Related Factors): The cause(s) or contributing factors to the problem, indicated by “related to.”
- Defining Characteristics (Signs and Symptoms): The evidence that the problem exists, indicated by “as evidenced by.”
For a detailed guide on formulating nursing diagnoses, refer to resources specifically dedicated to nursing diagnosis, such as “Nursing Diagnosis (NDx): Complete Guide and List.” This step ensures that the care plan is targeted to the patient’s specific needs and responses.
Step 4: Setting Priorities
Setting priorities is a crucial step in nursing care planning, involving establishing a preferential order for addressing nursing diagnoses and interventions. This process ensures that the most critical patient needs are addressed first, optimizing care delivery and patient outcomes. In this step, the nurse, in collaboration with the patient, determines which identified problems require immediate attention and which can be addressed later.
Prioritization of nursing diagnoses can be based on several frameworks, with Maslow’s Hierarchy of Needs being a widely used model. Diagnoses are often categorized into high, medium, or low priority:
- High Priority: Life-threatening problems that require immediate intervention to maintain patient safety and physiological stability. These typically involve basic physiological needs like airway, breathing, and circulation (ABCs).
- Medium Priority: Problems that are not directly life-threatening but may cause significant discomfort or complications if not addressed in a timely manner. These may include safety and security needs, as well as some psychosocial needs.
- Low Priority: Problems that are important to the patient’s overall well-being but can be addressed after more urgent needs are met. These often relate to higher-level needs like self-esteem and self-actualization.
Maslow’s Hierarchy of Needs provides a useful framework for prioritizing care:
Maslow’s Hierarchy of Needs
-
Basic Physiological Needs: These are the most fundamental needs for survival and include:
- Nutrition (water and food)
- Elimination (Toileting)
- Airway (suction)-breathing (oxygen)-circulation (pulse, cardiac monitor, blood pressure) (ABCs)
- Sleep
- Sex
- Shelter
- Exercise
These physiological needs form the base of Maslow’s pyramid and must be met first. Nursing diagnoses related to these needs take top priority.
-
Safety and Security: Once physiological needs are met, safety and security become priorities. These include:
- Injury prevention (side rails, call lights, hand hygiene, isolation, suicide precautions, fall precautions, car seats, helmets, seat belts)
- Fostering a climate of trust and safety (therapeutic relationship)
- Patient education (modifiable risk factors for stroke, heart disease).
Nursing diagnoses related to safety and security are of medium to high priority, depending on the patient’s specific situation.
-
Love and Belonging: These needs involve social connections and relationships:
- Foster supportive relationships
- Methods to avoid social isolation (bullying)
- Employ active listening techniques
- Therapeutic communication
- Sexual intimacy.
Nursing diagnoses in this category are typically medium priority, as social and emotional well-being are important for overall health.
-
Self-Esteem: These needs relate to feelings of self-worth and accomplishment:
- Acceptance in the community, workforce
- Personal achievement
- Sense of control or empowerment
- Accepting one’s physical appearance or body habitus.
Nursing diagnoses related to self-esteem are generally medium to low priority, focusing on long-term well-being.
-
Self-Actualization: This is the highest level of needs, focusing on personal growth and fulfillment:
- Empowering environment
- Spiritual growth
- Ability to recognize the point of view of others
- Reaching one’s maximum potential.
Nursing diagnoses addressing self-actualization are typically low priority in acute care settings but become more relevant in long-term care and rehabilitation.
Virginia Henderson’s 14 Needs as applied to Maslow’s Hierarchy of Needs. Learn more about it here.
When assigning priorities to nursing diagnoses, nurses must consider the patient’s health values, beliefs, available resources, and the urgency of the situation. Actively involving the patient in this prioritization process enhances patient cooperation and ensures that the care plan aligns with their needs and preferences.
Step 5: Establishing Client Goals and Desired Outcomes
After prioritizing nursing diagnoses, the next step is to establish client goals and desired outcomes for each diagnosis. Goals are broad statements describing the overall desired change in patient health status. Desired outcomes are specific, measurable, achievable, relevant, and time-bound (SMART) criteria that indicate when a goal has been met. Goals and outcomes provide direction for planning nursing interventions and serve as benchmarks for evaluating patient progress and the effectiveness of the care plan in addressing the identified nursing diagnoses.
Examples of goals and desired outcomes. Notice how they’re formatted and written.
For each nursing diagnosis, one overall goal is typically established. The terms “goal outcomes” and “expected outcomes” are often used interchangeably.
Effective goals and outcomes should be SMART, as outlined by Hamilton and Price (2013):
- Specific: Goals and outcomes should be clearly defined and focused, leaving no room for ambiguity.
- Measurable or Meaningful: Outcomes must be quantifiable and observable, allowing for objective assessment of progress.
- Attainable or Action-Oriented: Goals should be realistic and achievable for the patient, considering their current health status, resources, and motivation.
- Realistic or Results-Oriented: Goals should be relevant to the patient’s needs and values, and focused on achieving meaningful results for the patient’s health and well-being.
- Timely or Time-Oriented: Outcomes should have a specific timeframe for achievement, providing a sense of urgency and allowing for timely evaluation of progress.
Hogston (2011) suggests using the REEPIG standards to ensure high-quality care planning:
- Realistic: Goals and outcomes must be achievable given the available resources, patient capabilities, and healthcare environment.
- Explicitly Stated: Goals and outcomes should be clearly and precisely written, avoiding vague language and ensuring that everyone understands what needs to be achieved.
- Evidence-Based: Interventions chosen to achieve goals and outcomes should be supported by research evidence and best practices.
- Prioritized: Goals and outcomes should align with the prioritized nursing diagnoses, ensuring that the most critical needs are addressed first.
- Involve: The care planning process should actively involve the patient and, when appropriate, family members and other members of the multidisciplinary healthcare team.
- Goal-Centered: The entire care plan, including nursing diagnoses, interventions, and evaluation, should be focused on achieving the established patient goals and desired outcomes.
Short-Term and Long-Term Goals
Goals and expected outcomes can be classified as short-term or long-term, depending on the timeframe for achievement and the nature of the patient’s health needs. Both types are essential for comprehensive care planning and should be directly linked to the nursing diagnoses.
- Short-Term Goals: These are objectives that are expected to be achieved relatively quickly, typically within hours to days. Short-term goals are particularly relevant in acute care settings where the focus is on addressing immediate health problems and stabilizing the patient’s condition.
- Long-Term Goals: These are objectives that are expected to be achieved over a longer period, usually weeks to months. Long-term goals are common for patients with chronic conditions, those in rehabilitation, or those requiring ongoing care at home or in extended-care facilities. Discharge planning often involves setting long-term goals to ensure continued progress and problem resolution after the patient leaves the acute care setting.
Components of Goals and Desired Outcomes
Well-written goals and desired outcome statements typically include four key components:
Components of goals and desired outcomes in a nursing care plan.
- Subject: The subject is the individual receiving care, which is usually the patient. It can also refer to a specific part of the patient (e.g., leg, lungs) or an attribute (e.g., temperature, blood pressure). In most cases, the subject is assumed to be the patient unless otherwise specified (e.g., family member, caregiver).
- Verb: The verb describes the action the patient is expected to perform or demonstrate. It should be an action verb that is observable and measurable (e.g., verbalize, demonstrate, walk, maintain).
- Conditions or Modifiers: These elements specify the circumstances under which the behavior is to be performed. They clarify “what,” “when,” “where,” or “how” the patient will achieve the outcome. Conditions add detail and context to the outcome statement.
- Criterion of Desired Performance: The criterion defines the standard or level of performance expected for the outcome. It specifies how well the patient needs to perform the behavior to be considered successful. Criteria should be measurable and realistic.
When writing goals and desired outcomes, consider these tips to ensure effectiveness and relevance to the nursing diagnoses:
- Frame goals and outcomes in terms of patient responses, not nursing activities. Begin each goal with “Client will […]” to maintain a patient-centered focus.
- Avoid stating goals as what the nurse hopes to achieve; instead, focus on what the patient will do or achieve as a result of nursing care.
- Use observable and measurable terms for outcomes. Avoid vague words that are open to interpretation or subjective judgment.
- Ensure desired outcomes are realistic for the patient’s resources, capabilities, limitations, and the designated timeframe for care.
- Verify that goals and outcomes are compatible with the overall treatment plan and therapies provided by other healthcare professionals.
- Ensure each goal is derived from only one nursing diagnosis. This clarity facilitates evaluation by ensuring that interventions are directly related to the identified diagnosis.
- Finally, confirm that the patient considers the goals important and values them. Patient involvement and agreement are essential for cooperation and successful goal achievement.
Step 6: Selecting Nursing Interventions
Nursing interventions are the specific actions that nurses perform to help patients achieve their goals and desired outcomes, and ultimately resolve the nursing diagnoses. Interventions should be evidence-based, tailored to the individual patient’s needs and preferences, and directly address the etiology or risk factors of the identified nursing diagnosis. Interventions are identified and documented during the planning phase of the nursing process but are actually carried out during the implementation phase.
Types of Nursing Interventions
Nursing interventions can be categorized into three main types: independent, dependent, and collaborative:
Types of nursing interventions in a care plan.
-
Independent Nursing Interventions: These are actions that nurses are licensed to initiate based on their professional judgment and skills. They do not require a physician’s order. Examples include:
- Ongoing patient assessment and monitoring
- Providing emotional support and counseling
- Offering comfort measures
- Patient education and health teaching
- Providing physical care and assistance with activities of daily living
- Making referrals to other healthcare professionals.
Independent interventions are crucial for addressing many nursing diagnoses and promoting patient well-being.
-
Dependent Nursing Interventions: These are actions that require a physician’s order or supervision to be implemented. They are carried out in response to medical diagnoses and treatments. Examples include:
- Administering medications
- Providing intravenous therapy and fluid management
- Performing diagnostic tests (e.g., ECG, blood draws)
- Implementing medical treatments (e.g., wound care, respiratory therapy)
- Managing diet and activity orders.
While dependent interventions are prescribed by physicians, nurses play a vital role in their safe and effective implementation, including assessment, monitoring, and patient education.
-
Collaborative Interventions: These are actions that nurses carry out in partnership with other members of the healthcare team, such as physicians, social workers, dietitians, physical therapists, and occupational therapists. Collaborative interventions are developed through interdisciplinary consultation and aim to provide holistic and coordinated care. Examples include:
- Participating in team conferences to plan patient care
- Working with physical therapists to develop rehabilitation plans
- Consulting with dietitians to manage nutritional needs
- Collaborating with social workers to address psychosocial and discharge planning needs.
Collaborative interventions are essential for addressing complex patient needs that require a multidisciplinary approach and integrated care planning.
Nursing interventions should adhere to the following criteria to ensure they are effective and patient-centered:
- Safe and Appropriate: Interventions must be safe for the patient and appropriate for their age, health condition, and overall status.
- Achievable and Realistic: Interventions should be feasible to implement given the available resources, time constraints, and patient capabilities.
- Aligned with Patient Values and Beliefs: Interventions should be compatible with the patient’s cultural background, values, and beliefs, respecting their autonomy and preferences.
- Consistent with Other Therapies: Interventions should complement and not conflict with other medical or therapeutic treatments the patient is receiving.
- Based on Nursing Knowledge and Evidence: Interventions should be grounded in established nursing knowledge, evidence-based practices, and relevant scientific principles. The rationale for each intervention should be clear and linked to the nursing diagnosis.
When documenting nursing interventions in the care plan, follow these tips for clarity and completeness:
- Date and sign the care plan. Dating the plan is essential for tracking its currency and for future review and evaluation. The nurse’s signature indicates accountability and responsibility for the plan.
- Write interventions that are specific and clearly stated, starting with an action verb that precisely describes what the nurse is expected to do. Action verbs should be precise and direct (e.g., “Administer,” “Educate,” “Assess,” “Monitor”). Include qualifiers that specify how, when, where, how often, and in what amount the intervention should be performed. For example: “Educate parents on how to take temperature and notify of any changes immediately,” or “Assess urine for color, amount, odor, and turbidity every shift.”
- Use only abbreviations that are approved and accepted by the healthcare institution to avoid confusion and potential errors in communication.
Step 7: Providing Rationale
Rationales, also known as scientific explanations, are a critical component of student nursing care plans. They explain the scientific basis for each nursing intervention, linking the intervention back to the nursing diagnosis and desired outcome. Rationales demonstrate the student’s understanding of the underlying pathophysiology, pharmacology, or psychological principles that justify the chosen interventions.
Sample nursing interventions and rationale for a care plan (NCP)
Rationales are typically not included in care plans used by practicing nurses in clinical settings, as it is assumed that professional nurses understand the scientific basis for their interventions. However, for nursing students, writing rationales is an invaluable learning exercise that reinforces the connection between nursing theory and practice. By articulating the rationale, students develop a deeper understanding of why specific interventions are effective and how they contribute to achieving patient outcomes and resolving nursing diagnoses.
Step 8: Evaluation
Evaluation is the final, but ongoing, step in the nursing process and care planning. It is a planned, systematic, and continuous activity in which the nurse assesses the patient’s progress toward achieving the established goals and desired outcomes. Evaluation also involves determining the effectiveness of the nursing care plan in addressing the identified nursing diagnoses and making necessary revisions to the plan as needed.
Evaluation is a critical aspect of the nursing process because the conclusions drawn from this step determine whether the nursing care plan should be:
- Terminated: If the patient has achieved all goals and desired outcomes, and the nursing diagnoses have been resolved, the care plan may be terminated.
- Continued: If the patient is making progress but has not yet fully achieved the goals, the care plan may be continued with the same interventions.
- Modified: If the patient is not progressing as expected, or if new nursing diagnoses have emerged, the care plan needs to be revised. Modifications may involve changing interventions, adjusting goals, or addressing new problems.
The evaluation process typically involves:
- Reassessing the Patient: Gathering updated data to determine the patient’s current health status and response to interventions.
- Comparing Data to Outcomes: Analyzing the reassessment data to determine if the patient has achieved the desired outcomes specified in the care plan.
- Analyzing Goal Achievement: Making a judgment about the extent to which each goal has been met (e.g., goal met, partially met, not met).
- Identifying Factors Affecting Outcomes: Determining factors that have contributed to or hindered goal achievement.
- Modifying the Care Plan: Based on the evaluation, revising the care plan as needed to improve its effectiveness and better meet the patient’s evolving needs and nursing diagnoses.
- Documenting Evaluation: Recording the evaluation findings, including the patient’s progress, goal achievement, and any modifications made to the care plan.
Step 9: Putting it on Paper
The final step in the care planning process is documenting the care plan in the patient’s medical record. The format and specific requirements for documentation may vary depending on hospital policy and the healthcare setting. The documented care plan becomes a permanent part of the patient’s medical record and serves as a communication tool for all members of the healthcare team, especially for oncoming nurses during shift changes. Clear and accurate documentation of nursing diagnoses, goals, interventions, and evaluation is essential for ensuring continuity of care and demonstrating professional accountability.
Different nursing programs and healthcare agencies may use various care plan formats. Many formats are structured to guide students and nurses systematically through the interrelated steps of the nursing process, often using a multi-column format to organize the information clearly and logically.
Nursing Care Plan List
This section provides a list of sample nursing care plans (NCPs) and nursing diagnoses for a wide range of diseases and health conditions. These care plans are categorized by clinical specialty to help nurses quickly find relevant resources. Each care plan example is designed to illustrate the application of the nursing process and the integration of nursing diagnoses into patient care.
(List of Nursing Care Plans Categories and links from the original article – already provided in the prompt)
Recommended Resources
Recommended nursing diagnosis and nursing care plan books and resources.
Disclosure: Included below are affiliate links from Amazon at no additional cost from you. We may earn a small commission from your purchase. For more information, check out our privacy policy.
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning CareWe love this book because of its evidence-based approach to nursing interventions. This care plan handbook uses an easy, three-step system to guide you through client assessment, nursing diagnosis, and care planning. Includes step-by-step instructions showing how to implement care and evaluate outcomes, and help you build skills in diagnostic reasoning and critical thinking.
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition)Includes over two hundred care plans that reflect the most recent evidence-based guidelines. New to this edition are ICNP diagnoses, care plans on LGBTQ health issues, and on electrolytes and acid-base balance.
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales Quick-reference tool includes all you need to identify the correct diagnoses for efficient patient care planning. The sixteenth edition includes the most recent nursing diagnoses and interventions and an alphabetized listing of nursing diagnoses covering more than 400 disorders.
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care Identify interventions to plan, individualize, and document care for more than 800 diseases and disorders. Only in the Nursing Diagnosis Manual will you find for each diagnosis subjectively and objectively – sample clinical applications, prioritized action/interventions with rationales – a documentation section, and much more!
All-in-One Nursing Care Planning Resource – E-Book: Medical-Surgical, Pediatric, Maternity, and Psychiatric-Mental Health Includes over 100 care plans for medical-surgical, maternity/OB, pediatrics, and psychiatric and mental health. Interprofessional “patient problems” focus familiarizes you with how to speak to patients.
References and Sources
Recommended reading materials and sources for this NCP guide: