What is a Nursing Care Plan?
A Nursing Care Plan (NCP) is a structured methodology utilized by nurses to pinpoint patient needs, both current and potential. It serves as a vital communication tool among nurses, patients, and the broader healthcare team, ensuring cohesive and goal-oriented patient care. The NCP is crucial for maintaining consistency and quality in healthcare delivery, acting as a roadmap to guide nursing actions and achieve desired patient outcomes. Without a well-defined nursing care plan, patient care can become fragmented and less effective.
The process of nursing care planning is dynamic, commencing at the point of patient admission and undergoing continuous refinement. This ongoing adaptation is essential to reflect changes in the patient’s condition and to evaluate the effectiveness of interventions in meeting established goals. At its core, nursing care planning champions individualized, patient-centered care, which is the hallmark of excellent nursing practice.
Types of Nursing Care Plans
Nursing care plans exist on a spectrum from informal to formal. An informal nursing care plan is essentially a mental strategy, a nurse’s internal roadmap for patient care. In contrast, a formal nursing care plan is a documented, either written or electronic, guide that systematically organizes patient information and care strategies.
Formal care plans are further categorized into standardized and individualized approaches. Standardized care plans are pre-designed frameworks that address the common needs of patient groups with similar conditions. Individualized care plans, on the other hand, are meticulously tailored to address the specific and unique needs of each patient, going beyond the scope of standardized plans.
Standardized Care Plans
Standardized care plans are pre-established protocols developed by nursing staff and healthcare institutions. They are designed to guarantee consistent care for patients with specific, recurring conditions. These plans serve to establish a baseline of acceptable care and enhance efficiency by eliminating the need to repeatedly create plans for common patient needs within a nursing unit.
While standardized care plans are not customized to individual patient goals, they are invaluable as a foundation for developing a more personalized individualized care plan.
The care plans referenced in this guide are primarily standardized, intended to serve as a starting point or framework for creating individualized care plans.
Individualized Care Plans
An individualized care plan is developed by adapting a standardized plan to align with the unique needs and goals of a specific patient. This involves incorporating approaches known to be particularly effective for that individual. This method promotes more personalized and holistic care, better suited to the patient’s unique circumstances, strengths, and aspirations.
Moreover, individualized care plans are known to enhance patient satisfaction. When patients perceive that their care is specifically designed for them, they feel more valued and understood. This heightened sense of satisfaction is increasingly important in the contemporary healthcare environment, where patient satisfaction metrics are frequently used as indicators of care quality.
Tips for personalizing a nursing care plan:
Objectives
The primary objectives of creating nursing care plans include:
- To foster evidence-based nursing practice, ensuring a high standard of care within hospitals and healthcare facilities.
- To promote holistic care, addressing the patient’s physical, psychological, social, and spiritual dimensions in disease management and prevention.
- To establish structured care protocols such as care pathways and care bundles. Care pathways facilitate team consensus on care standards and expected outcomes, while care bundles focus on best practices for specific conditions.
- To clearly define and differentiate between goals and expected outcomes in patient care.
- To enhance communication and documentation of care plans, ensuring clarity and accessibility for all healthcare providers.
- To provide a framework for measuring and evaluating the effectiveness of nursing care interventions.
Purposes of a Nursing Care Plan
Nursing care plans serve several critical purposes in healthcare, emphasizing their importance:
- Defining the Nurse’s Role: Care plans delineate the distinct and autonomous role of nurses in addressing patients’ comprehensive health and well-being, beyond physician directives.
- Guiding Individualized Patient Care: They act as a blueprint for patient care, encouraging nurses to apply critical thinking to tailor interventions to individual needs.
- Ensuring Continuity of Care: By providing a consistent care framework, care plans enable nurses across different shifts and departments to deliver uniform, high-quality interventions, maximizing treatment benefits for patients.
- Coordinating Care: Care plans ensure all members of the healthcare team are informed of patient needs and the necessary actions, preventing gaps in care and promoting a unified approach.
- Documentation: They serve as accurate records of planned observations, nursing actions, and patient/family instructions. Proper documentation in the care plan is essential to verify that care was provided.
- Staff Assignment Guidance: Care plans can inform staff assignments, ensuring patients are cared for by nurses with the appropriate skills for their specific needs.
- Monitoring Progress: They facilitate the tracking of patient progress and allow for necessary adjustments to the care plan in response to evolving health status and goals.
- Supporting Reimbursement: Insurance providers utilize medical records, including care plans, to assess and determine coverage for hospital care.
- Defining Patient Goals: Care plans actively involve patients in their treatment, aligning care with their personal health goals and preferences.
Components
A typical Nursing Care Plan (NCP) encompasses several key components, including nursing diagnoses, patient problems, desired outcomes, nursing interventions, and rationales. Each of these elements is detailed below:
Care Plan Formats
Nursing care plans are often structured in formats that facilitate clarity and ease of use, commonly organized into three, four, or five-column layouts.
Three-Column Format
The three-column format is a streamlined approach, typically including columns for nursing diagnoses, outcomes/evaluation, and interventions.
Example of a 3-column nursing care plan format, showing the integration of nursing diagnosis, outcomes, evaluation, and interventions for efficient care planning.
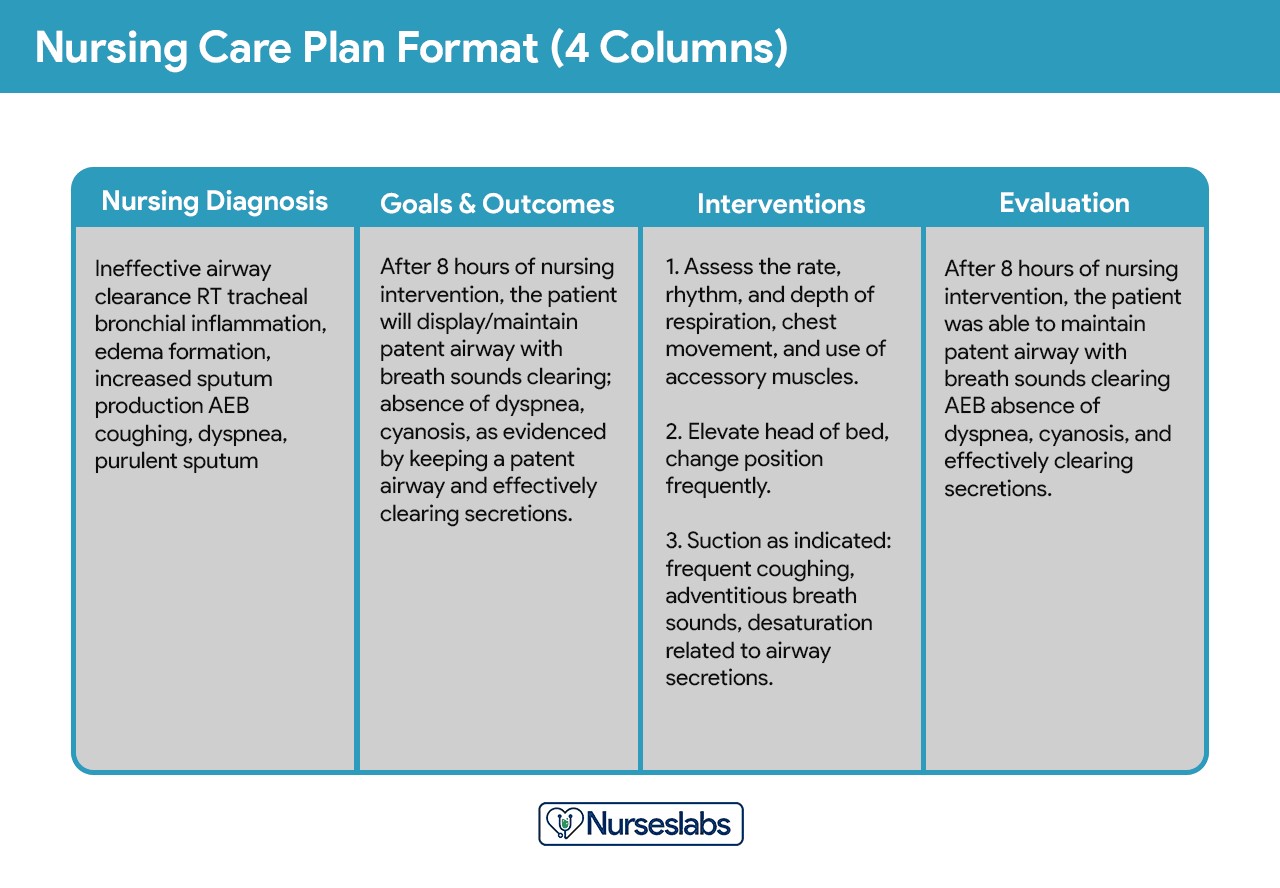
Four-Column Format
This format expands on the three-column structure by separating outcomes and evaluation into distinct columns, providing enhanced detail and clarity. The columns typically include nursing diagnosis, goals/outcomes, interventions, and evaluation.
Example of a 4-column nursing care plan template, illustrating a detailed structure for nursing diagnosis, goals, interventions, and evaluation to facilitate comprehensive patient care.
For practical use, sample templates for various nursing care plan formats are available for download, modification, and distribution:
Download: Printable Nursing Care Plan Templates and Formats
Student Care Plans
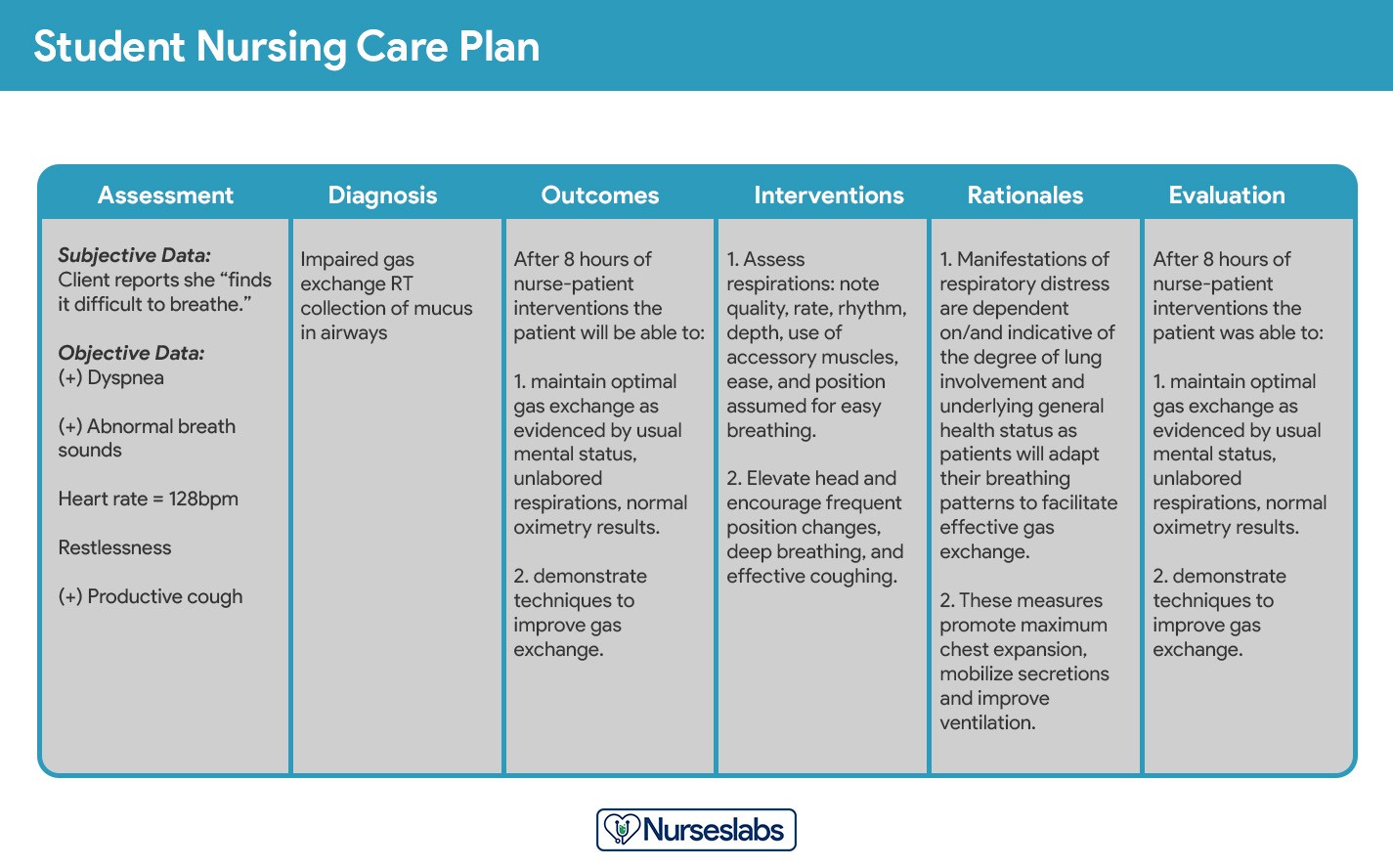
Student care plans are designed to be more comprehensive and detailed than those used by practicing nurses. They serve as a crucial learning tool for nursing students, helping them develop critical thinking and care planning skills.
Example of a student nursing care plan format, designed for educational purposes with enhanced detail and rationales to support learning and comprehensive patient care planning.
Often, student care plans are handwritten and include an additional column for “Rationale” or “Scientific Explanation,” which follows the nursing interventions column. Rationales provide the scientific basis for each nursing intervention, linking actions to physiological or psychological principles.
Writing a Nursing Care Plan
Creating an effective Nursing Care Plan (NCP) involves a systematic approach. Follow these steps to develop a comprehensive care plan for your patient:
Step 1: Data Collection or Assessment
The initial step in formulating a nursing care plan is compiling a comprehensive patient database. This is achieved through thorough assessment techniques and data collection methods, including physical assessments, detailed health histories, patient interviews, reviews of medical records, and diagnostic studies. This database encompasses all relevant health information gathered about the patient. During this phase, nurses identify pertinent related or risk factors and defining characteristics that will inform the nursing diagnoses. Specific assessment formats may be mandated by healthcare agencies or nursing schools.
Critical thinking is paramount in patient assessment, integrating scientific knowledge and professional guidelines to inform evaluations. This process, essential for complex clinical decision-making, aims to effectively identify patients’ healthcare needs within a supportive environment and using reliable information.
Step 2: Data Analysis and Organization
Once patient health information is collected, the next step is to analyze, categorize, and organize this data. This structured analysis is crucial for formulating accurate nursing diagnoses, establishing care priorities, and defining desired patient outcomes.
Step 3: Formulating Your Nursing Diagnoses
Nursing diagnoses are standardized statements that identify specific patient needs and responses to health conditions or life processes. They focus on actual and potential health problems that nurses can address through independent nursing interventions.
For detailed guidance on formulating nursing diagnoses, refer to this resource: Nursing Diagnosis (NDx): Complete Guide and List.
Step 4: Setting Priorities
Setting priorities involves ranking nursing diagnoses and interventions in order of importance. This step requires nurses to collaborate with patients to determine which identified problems require immediate attention. Diagnoses are typically categorized as high, medium, or low priority, with life-threatening issues taking precedence.
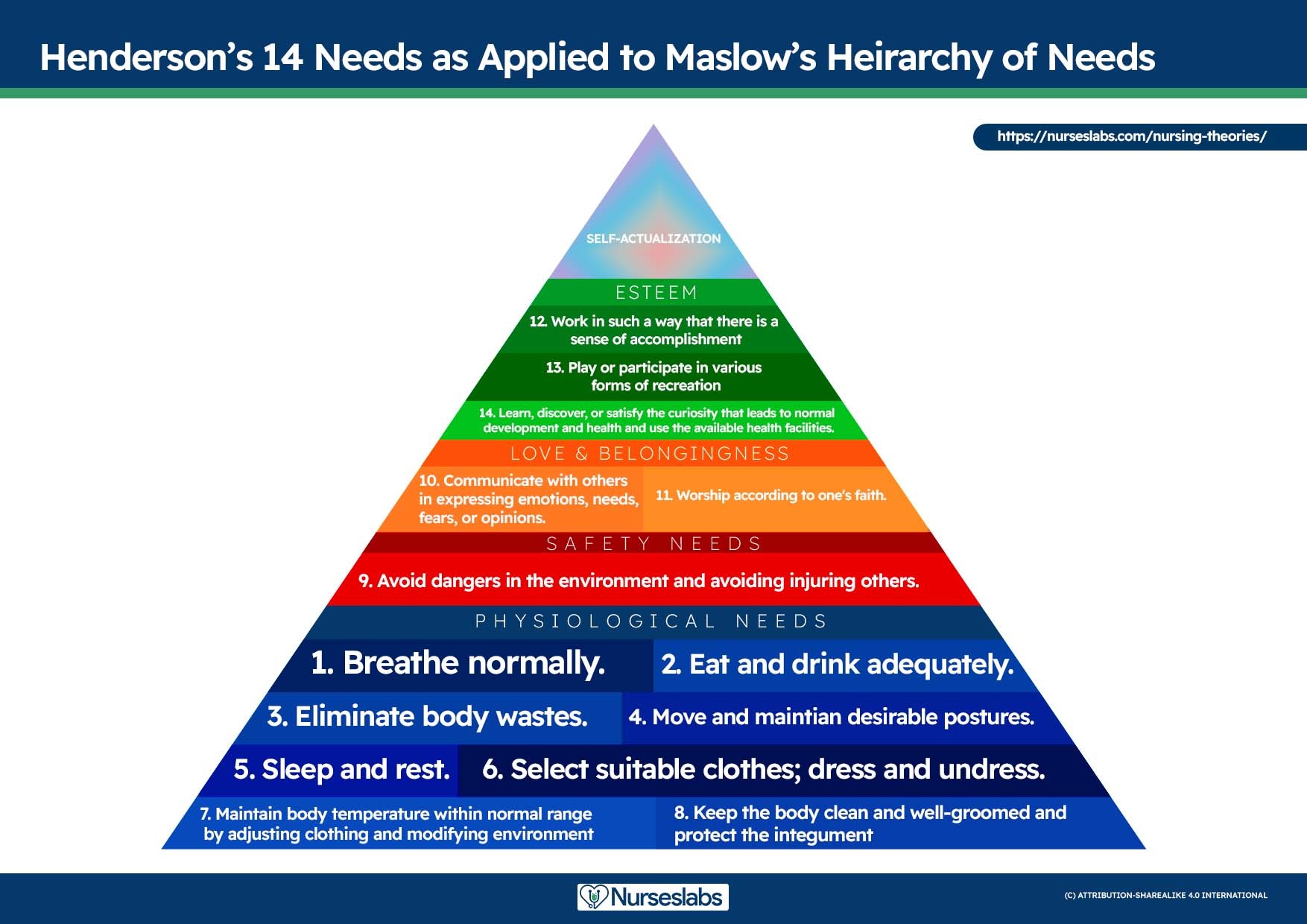
Nursing diagnoses are inherently linked to Maslow’s Hierarchy of Needs, a framework that helps prioritize care based on fundamental human needs. Developed by Abraham Maslow in 1943, this hierarchy posits that basic physiological needs must be met before higher-level needs, such as self-esteem and self-actualization, can be addressed. Physiological and safety needs are foundational to nursing care and interventions, forming the base of Maslow’s pyramid and underpinning physical and emotional well-being.
Maslow’s Hierarchy of Needs
- Basic Physiological Needs: These include essential survival needs such as nutrition (water and food), elimination, airway management (suctioning), breathing support (oxygen), circulation monitoring (pulse, cardiac monitoring, blood pressure), sleep, sexual health, shelter, and exercise.
- Safety and Security: This level focuses on injury prevention (side rails, call lights, hand hygiene, isolation protocols, suicide precautions, fall prevention, car seats, helmets, seat belts) and creating a safe and trusting environment (therapeutic relationships), including patient education on modifiable risk factors for conditions like stroke and heart disease.
- Love and Belonging: Addressing social needs through fostering supportive relationships, preventing social isolation (bullying intervention), employing active listening, therapeutic communication, and supporting healthy sexual intimacy.
- Self-Esteem: Promoting self-acceptance within the community and workplace, recognizing personal achievements, fostering a sense of control and empowerment, and accepting one’s physical appearance.
- Self-Actualization: Creating an empowering environment that supports spiritual growth and the ability to understand diverse perspectives, enabling individuals to reach their full potential.
Virginia Henderson’s 14 Needs applied to Maslow’s Hierarchy of Needs, demonstrating the integration of fundamental nursing principles with a well-established framework for understanding human needs and prioritizing patient care. Learn more about it here.
When prioritizing care, nurses must consider the patient’s health values, beliefs, available resources, and the urgency of the situation. Patient involvement in this process is crucial to foster cooperation and adherence to the care plan.
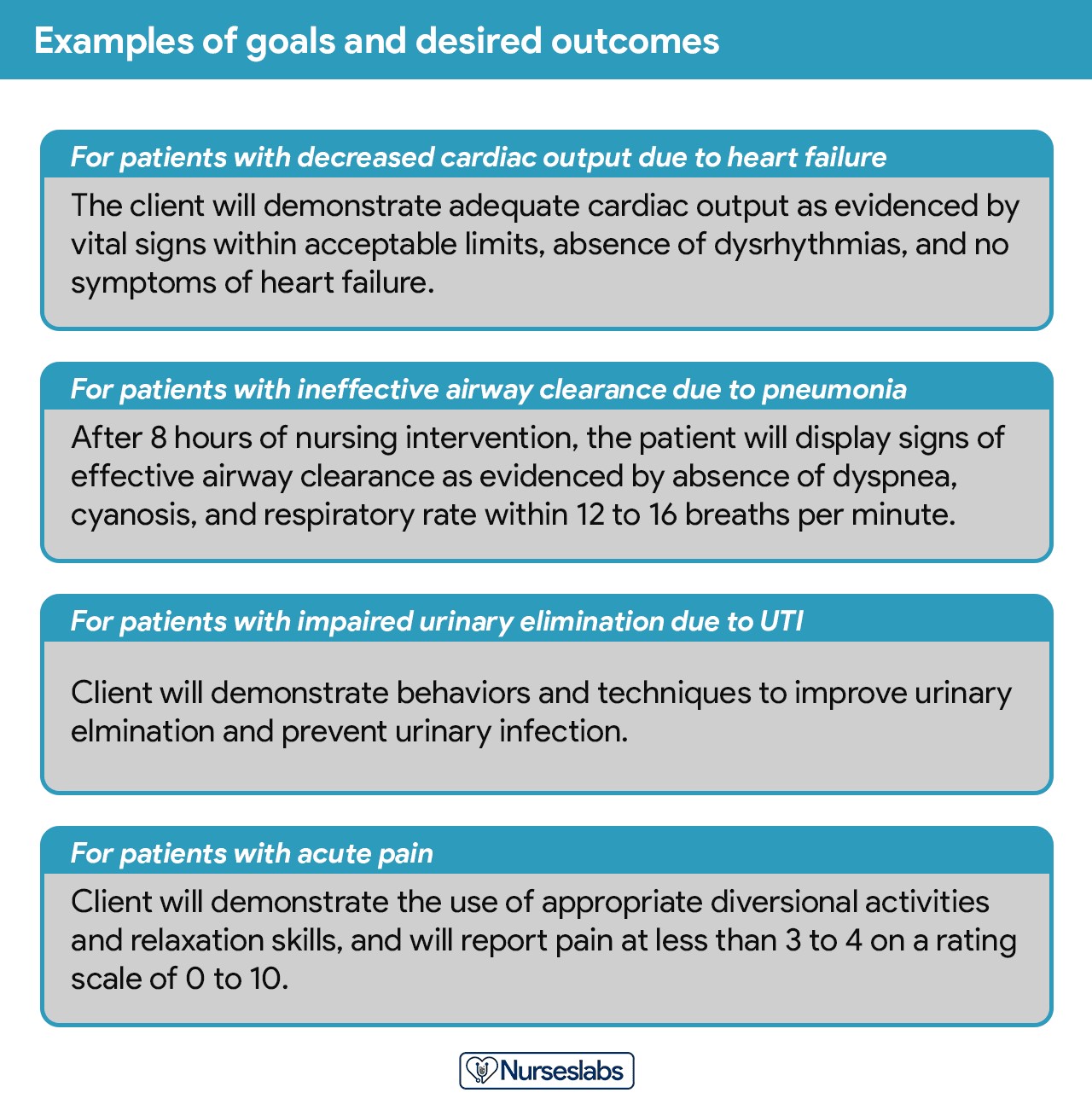
Step 5: Establishing Client Goals and Desired Outcomes
Following the prioritization of nursing diagnoses, nurses collaborate with patients to set goals for each identified priority. Goals or desired outcomes articulate the intended results of nursing interventions, derived from the patient’s nursing diagnoses. These goals guide intervention planning, provide benchmarks for evaluating patient progress, help both patient and nurse identify problem resolution, and enhance motivation by providing a sense of accomplishment.
Examples of well-formulated goals and desired outcomes in nursing care plans, illustrating how they are structured and written to be specific, measurable, achievable, relevant, and time-bound.
A primary goal is established for each nursing diagnosis. The terms “goal outcomes” and “expected outcomes” are often used interchangeably.
Effective goals should adhere to the SMART criteria, as outlined by Hamilton and Price (2013): Specific, Measurable, Attainable, Realistic, and Time-oriented.
- Specific: Goals should be clearly defined, significant, and directly relevant to the patient’s needs.
- Measurable: Measurability allows for objective tracking of progress and determination of goal achievement.
- Attainable: Goals should be challenging yet achievable, within the patient’s capabilities and circumstances.
- Realistic: Goals must be practical and consider available resources and the patient’s overall situation.
- Time-Oriented: Each goal should have a defined timeframe, providing a sense of urgency and a target for progress.
Hogston (2011) suggests using the REEPIG standards to ensure high-quality care plans: Realistic, Explicitly stated, Evidence-based, Prioritized, Involve, and Goal-centered.
- Realistic: Goals must be achievable given the available resources.
- Explicitly stated: Instructions must be clear and unambiguous to prevent misinterpretations.
- Evidence-based: Interventions should be supported by current research and best practices.
- Prioritized: The most critical problems should be addressed first.
- Involve: Care planning should include both the patient and all relevant members of the multidisciplinary team.
- Goal-centered: Planned care must directly contribute to achieving the established goals.
Short-Term and Long-Term Goals
Goals and expected outcomes must be measurable and patient-centered, focusing on problem prevention, resolution, and rehabilitation. Goals are classified as short-term or long-term. In acute care settings, most goals are short-term, addressing immediate patient needs. Long-term goals are more common for patients with chronic conditions or those in long-term care facilities.
- Short-term goal: A statement of expected change achievable in a short period, typically hours to days.
- Long-term goal: An objective to be achieved over a longer duration, usually weeks to months.
- Discharge planning: Primarily involves setting long-term goals to ensure ongoing restorative care and problem resolution through home health services, physical therapy, or other referrals.
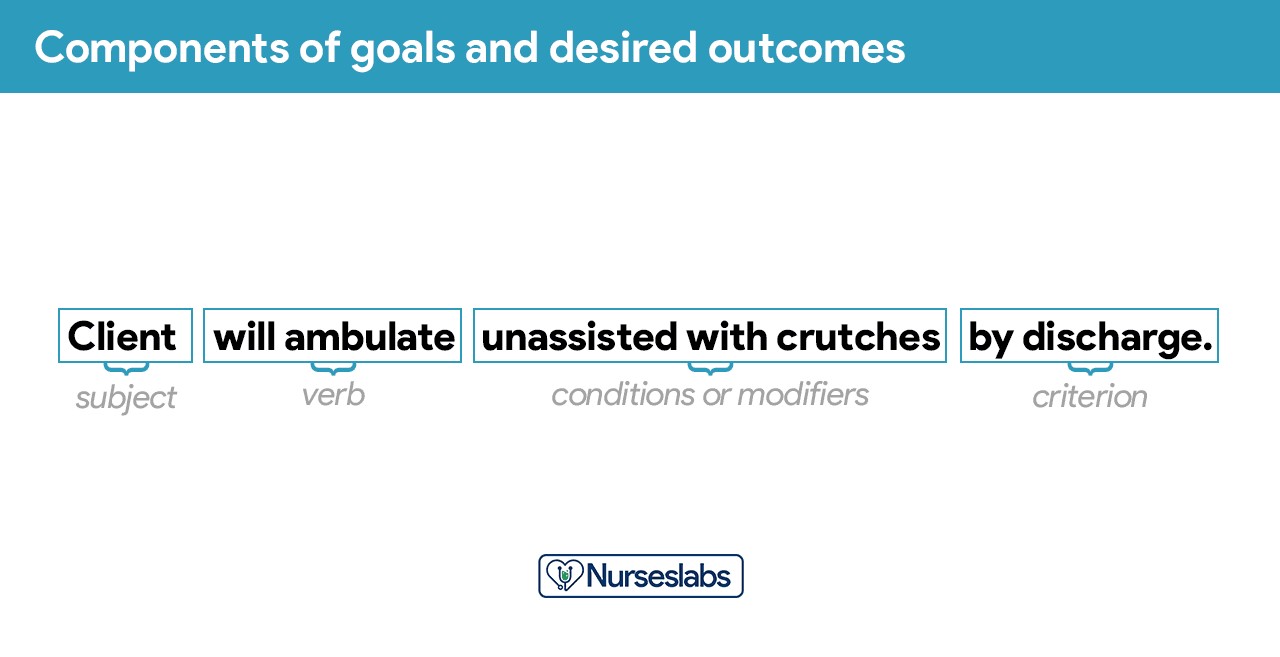
Components of Goals and Desired Outcomes
Goal and desired outcome statements typically include four components: a subject, a verb, conditions/modifiers, and a criterion of desired performance.
Breakdown of the components of goals and desired outcomes in a nursing care plan, detailing the subject, verb, conditions, and criteria necessary for well-defined and effective goal setting.
- Subject: Usually the patient, a part of the patient, or a patient attribute (e.g., pulse rate, temperature, urinary output). Often implied as the patient unless otherwise specified (e.g., family, caregiver).
- Verb: Specifies the action the patient is expected to perform, learn, or experience.
- Conditions or modifiers: Detail the circumstances under which the behavior should occur (what, when, where, how).
- Criterion of desired performance: Defines the standard for evaluating performance or the level of behavior expected. This component is optional but enhances goal clarity.
When formulating goals and desired outcomes, nurses should consider these guidelines:
- Frame goals and outcomes in terms of patient responses, not nursing activities. Start each goal with “Client will […]” to maintain focus on patient behavior and outcomes.
- Avoid focusing on what the nurse hopes to achieve; instead, emphasize what the patient will do.
- Use observable and measurable terms for outcomes, avoiding vague language that requires subjective interpretation.
- Ensure desired outcomes are realistic given the patient’s resources, abilities, limitations, and the care timeframe.
- Verify that goals are compatible with other therapeutic interventions from other healthcare professionals.
- Ensure each goal is derived from a single nursing diagnosis to facilitate clear evaluation of care and ensure interventions are directly linked to the diagnosis.
- Finally, confirm that the patient values and considers the goals important to ensure their active participation and cooperation.
Step 6: Selecting Nursing Interventions
Nursing interventions are the specific actions nurses will perform to help patients achieve their goals. Interventions should aim to eliminate or alleviate the root causes of the prioritized nursing problem or diagnosis. For risk diagnoses, interventions should focus on mitigating risk factors. While nursing interventions are identified and documented during the planning phase of the nursing process, they are actually carried out during the implementation phase.
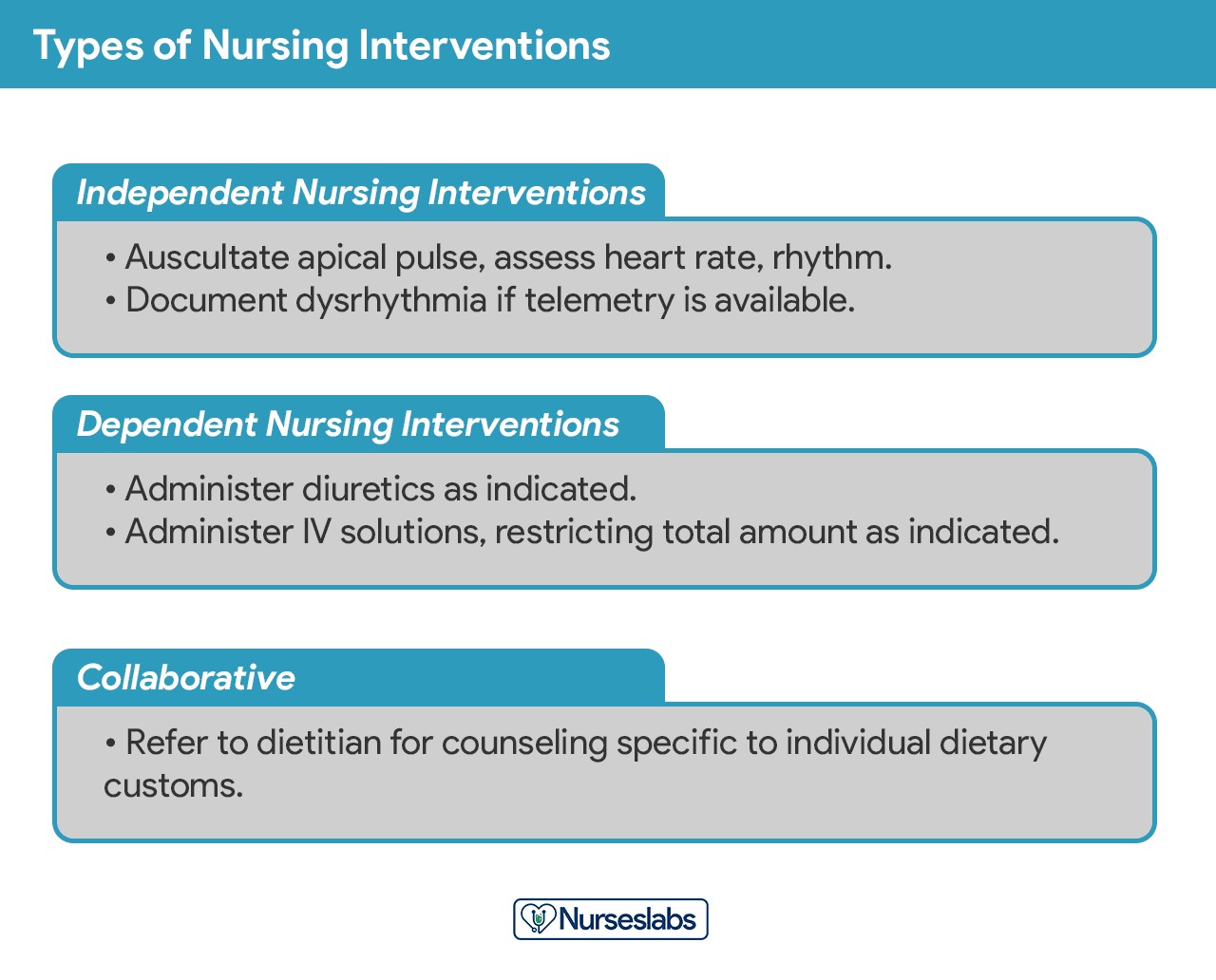
Types of Nursing Interventions
Nursing interventions can be categorized as independent, dependent, or collaborative:
Classification of nursing interventions in a care plan, outlining independent, dependent, and collaborative actions to provide a comprehensive approach to patient care.
- Independent nursing interventions are actions nurses are authorized to initiate based on their professional judgment and skills. These include ongoing assessments, emotional support, providing comfort, patient education, physical care, and referrals to other healthcare providers.
- Dependent nursing interventions are actions implemented under the orders or supervision of a physician. These encompass medication administration, intravenous therapy, diagnostic tests, treatments, dietary orders, and activity or rest directives. Nurses also play a role in assessment and patient education related to these medical orders.
- Collaborative interventions are actions nurses undertake in partnership with other healthcare team members, such as physicians, social workers, dietitians, and therapists. These interventions are developed through consultation to integrate diverse professional perspectives.
Nursing interventions should be:
- Safe and appropriate for the patient’s age, health status, and condition.
- Achievable given available resources and time constraints.
- Consistent with the patient’s values, cultural background, and beliefs.
- Compatible with other planned therapies.
- Based on established nursing knowledge, experience, and relevant scientific principles.
When documenting nursing interventions, adhere to these guidelines:
- Date and sign the care plan. Dating is essential for tracking, reviewing, and updating the plan. The nurse’s signature confirms accountability.
- Nursing interventions should be specific and clearly written, starting with an action verb that indicates the expected nurse action. Action verbs should be precise, and qualifiers specifying how, when, where, time, frequency, and amount should provide context for the planned activity. For example: “Educate parents on how to measure temperature and report any changes,” or “Assess urine for color, volume, odor, and clarity.”
- Use only institution-approved abbreviations.
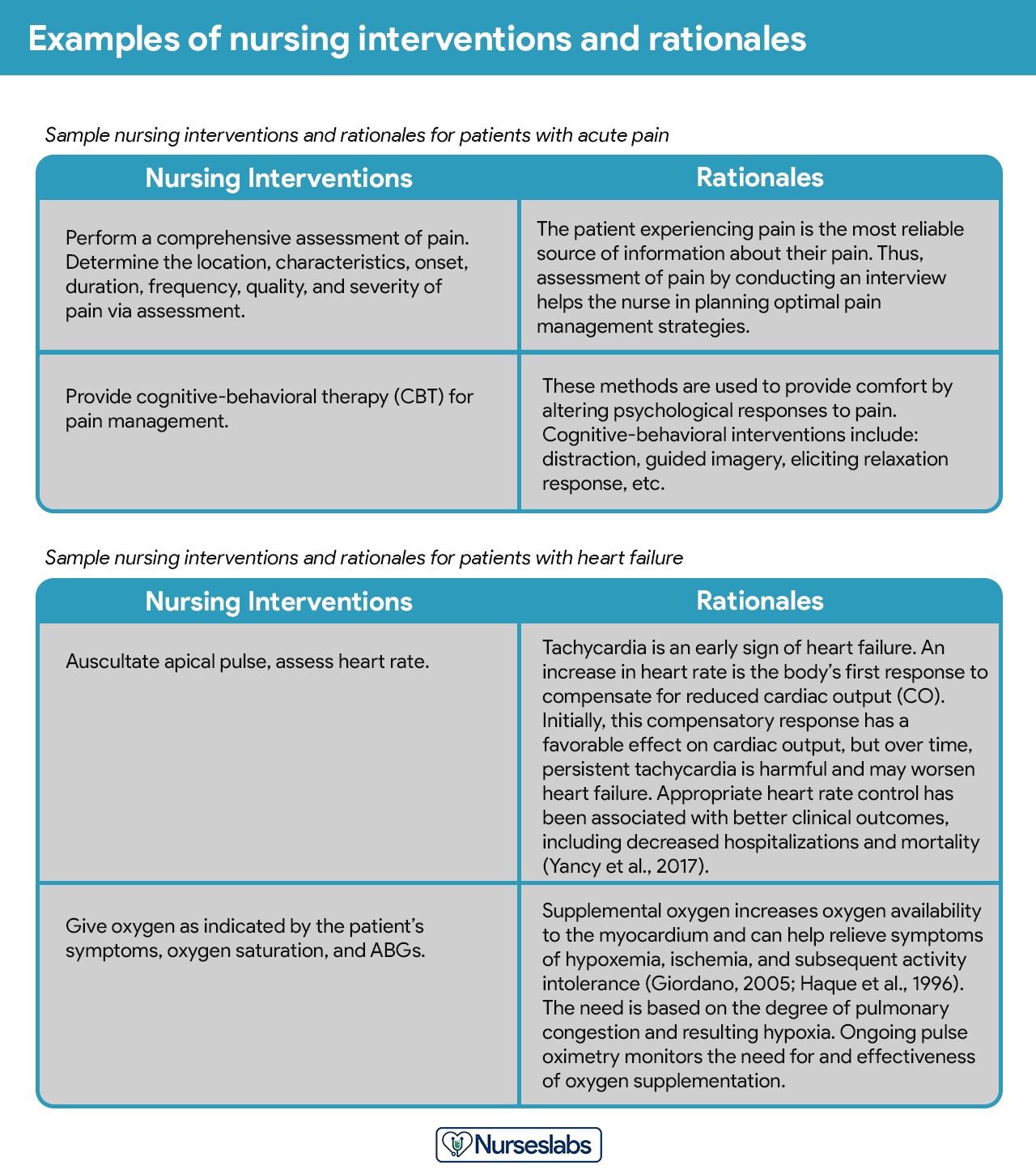
Step 7: Providing Rationale
Rationales, or scientific explanations, justify the selection of each nursing intervention within the NCP.
Example of nursing interventions paired with rationales in a care plan, illustrating the scientific basis and justification for chosen nursing actions to enhance understanding and effective care delivery.
Rationales are typically included in student care plans to help nursing students link pathophysiological and psychological principles to their chosen nursing interventions. They are less commonly found in standard practice care plans.
Step 8: Evaluation
Evaluation is a systematic, ongoing, and purposeful process used to assess the patient’s progress toward achieving the set goals and to determine the effectiveness of the nursing care plan (NCP). This crucial step in the nursing process informs decisions about whether to continue, modify, or discontinue specific nursing interventions.
Step 9: Putting it on Paper
The finalized patient care plan is documented according to hospital policies and becomes a part of the patient’s permanent medical record, accessible for review by all members of the healthcare team. Nursing education programs often have specific care plan formats. Most formats are designed to guide students through the sequential steps of the nursing process, with many employing a five-column layout for comprehensive planning and documentation.
Nursing Care Plan List
This section provides a categorized list of sample nursing care plans (NCPs) and nursing diagnoses for a wide range of health conditions and diseases.
Basic Nursing and General Care Plans
This category includes diverse nursing care plan examples that do not fit into other specific categories:
| Basic Nursing & General Care Plans |
|---|
| Acute Confusion (Delirium) and Altered Mental Status |
| Acute Pain and Pain Management |
| Activity Intolerance and Generalized Weakness |
| Cancer (Oncology Nursing) |
| Caregiver Role Strain and Family Caregiver Support Systems |
| Chronic Confusion (Dementia) |
| End-of-Life Care (Hospice Care or Palliative) |
| Fall Risk and Fall Prevention |
| Fatigue and Lethargy |
| Geriatric Nursing (Older Adult) |
| Grieving and Loss |
| Hypothermia and Cold Injuries |
| Hyperthermia (Fever) |
| Impaired Swallowing (Dysphagia) |
| Insomnia and Sleep Deprivation |
| Prolonged Bed Rest |
| Risk for Injury and Patient Safety |
| Self-Care and Activities of Daily Living (ADLs) |
| Surgery (Perioperative Client) |
| Systemic Lupus Erythematosus |
| Total Parenteral Nutrition |

Surgery and Perioperative Care Plans
Care plans specifically designed for patients undergoing surgical intervention:
| Surgery and Perioperative Care Plans |
|---|
| Amputation |
| Appendectomy |
| Cholecystectomy |
| Fracture UPDATED! |
| Hemorrhoids |
| Hysterectomy |
| Ileostomy & Colostomy |
| Laminectomy (Disc Surgery) |
| Mastectomy |
| Subtotal Gastrectomy |
| Surgery (Perioperative Client) |
| Thyroidectomy |
| Total Joint (Knee, Hip) Replacement |
Cardiac Care Plans
Nursing care plans addressing conditions related to the cardiovascular system:
| Cardiac Care Plans |
|---|
| Angina Pectoris (Coronary Artery Disease) |
| Cardiac Arrhythmia (Digitalis Toxicity) |
| Cardiac Catheterization |
| Cardiogenic Shock |
| Congenital Heart Disease |
| Decreased Cardiac Output & Cardiac Support |
| Heart Failure UPDATED! |
| Hypertension UPDATED! |
| Hypovolemic Shock |
| Impaired Tissue Perfusion & Ischemia |
| Myocardial Infarction |
| Pacemaker Therapy |
Endocrine and Metabolic Care Plans
Nursing care plans (NCPs) focused on the endocrine system and metabolic disorders:
| Endocrine and Metabolic Care Plans |
|---|
| Addison’s Disease |
| Cushing’s Disease |
| Diabetes Mellitus (Type 1, Type 2) UPDATED! |
| Diabetic Ketoacidosis (DKA) and Hyperglycemic Hyperosmolar Nonketotic Syndrome (HHNS) |
| Eating Disorders: Anorexia & Bulimia Nervosa |
| Fluid Volume Deficit (Dehydration & Hypovolemia) |
| Fluid Volume Excess (Hypervolemia) |
| Gestational Diabetes Mellitus |
| Hyperthyroidism |
| Hypothyroidism |
| Imbalanced Nutrition (Malnutrition) |
| Obesity & Overweight |
| Thyroidectomy |
| Unstable Blood Glucose Levels (Hyperglycemia & Hypoglycemia) |
| Acid-Base Imbalances |
|---|
| Metabolic Acidosis |
| Metabolic Alkalosis |
| Respiratory Acidosis |
| Respiratory Alkalosis |
| Electrolyte Imbalances |
|---|
| Calcium (Ca) Imbalances: Hypercalcemia and Hypocalcemia |
| Magnesium (Mg) Imbalances: Hypermagnesemia and Hypomagnesemia |
| Potassium (K) Imbalances: Hyperkalemia and Hypokalemia |
| Sodium (Na) Imbalances: Hypernatremia and Hyponatremia |
Gastrointestinal
Care plans (NCPs) covering disorders of the gastrointestinal and digestive system:
| Gastrointestinal Care Plans |
|---|
| Appendectomy |
| Bowel Incontinence (Fecal Incontinence) |
| Cholecystectomy |
| Constipation |
| Diarrhea Nursing Care Plan and Management |
| Cholecystitis and Cholelithiasis |
| Gastroenteritis |
| Gastroesophageal Reflux Disease (GERD) |
| Hemorrhoids |
| Hepatitis |
| Ileostomy & Colostomy |
| Inflammatory Bowel Disease (IBD) |
| Intussusception |
| Liver Cirrhosis |
| Nausea & Vomiting |
| Pancreatitis |
| Peritonitis |
| Peptic Ulcer Disease |
| Subtotal Gastrectomy |
| Umbilical and Inguinal Hernia |
Hematologic and Lymphatic
Care plans related to the hematologic and lymphatic system:
| Hematologic & Lymphatic Care Plans |
|---|
| Anaphylactic Shock |
| Anemia UPDATED! |
| Aortic Aneurysm |
| Bleeding Risk & Hemophilia |
| Deep Vein Thrombosis |
| Disseminated Intravascular Coagulation |
| Hemophilia |
| Kawasaki Disease |
| Leukemia |
| Lymphoma |
| Sepsis and Septicemia |
| Sickle Cell Anemia Crisis |
Infectious Diseases
NCPs for communicable and infectious diseases:
| Infectious Diseases Care Plans |
|---|
| Acquired Immunodeficiency Syndrome (AIDS) (HIV Positive) |
| Acute Rheumatic Fever |
| Dengue Hemorrhagic Fever |
| Herpes Zoster (Shingles) |
| Influenza (Flu) |
| Pulmonary Tuberculosis |
| Risk for Infection & Infection Control |
Integumentary
Comprehensive care plans for disorders and conditions affecting the integumentary system:
| Integumentary Care Plans |
|---|
| Burn Injury |
| Dermatitis |
| Herpes Zoster (Shingles) |
| Pressure Ulcer (Bedsores) |
| Wound Care and Skin/Tissue Integrity |
Maternal and Newborn Care Plans
Nursing care plans focused on the care of pregnant mothers and their newborns. Explore care plans for maternity and obstetric nursing:
| Maternal and Newborn Care Plans |
|---|
| Abortion (Termination of Pregnancy) |
| Cervical Insufficiency (Premature Dilation of the Cervix) |
| Cesarean Birth |
| Cleft Palate and Cleft Lip |
| Gestational Diabetes Mellitus |
| Hyperbilirubinemia (Jaundice) |
| Labor Stages, Induced, Augmented, Dysfunctional, Precipitous Labor |
| Neonatal Sepsis |
| Perinatal Loss (Miscarriage, Stillbirth) |
| Placental Abruption |
| Placenta Previa |
| Postpartum Hemorrhage |
| Postpartum Thrombophlebitis |
| Prenatal Hemorrhage |
| Preeclampsia and Gestational Hypertension |
| Prenatal Infection |
| Preterm Labor |
| Puerperal & Postpartum Infections |
| Substance (Alcohol and Drug) Abuse in Pregnancy |
Mental Health and Psychiatric
Care plans for mental health and psychiatric nursing:
| Mental Health and Psychiatric Care Plans |
|---|
| Alcohol Withdrawal |
| Anxiety & Fear |
| Anxiety and Panic Disorders |
| Bipolar Disorders |
| Body Image Disturbance & Self-Esteem |
| Impaired Thought Processes & Cognitive Impairment |
| Major Depression |
| Personality Disorders |
| Schizophrenia |
| Sexual Assault |
| Substance Dependence and Abuse |
| Suicide Behaviors |
Musculoskeletal
Care plans focused on conditions of the musculoskeletal system:
| Musculoskeletal Care Plans |
|---|
| Amputation |
| Congenital Hip Dysplasia |
| Fracture UPDATED! |
| Impaired Physical Mobility & Immobility |
| Juvenile Rheumatoid Arthritis |
| Laminectomy (Disc Surgery) |
| Osteoarthritis |
| Osteogenic Sarcoma (Osteosarcoma) |
| Osteoporosis |
| Rheumatoid Arthritis |
| Scoliosis |
| Spinal Cord Injury |
| Total Joint (Knee, Hip) Replacement |
Neurological
Nursing care plans (NCPs) for disorders related to the nervous system:
| Neurological Care Plans |
|---|
| Alzheimer’s Disease UPDATED! |
| Brain Tumor |
| Cerebral Palsy |
| Cerebrovascular Accident (Stroke) UPDATED! |
| Guillain-Barre Syndrome |
| Meningitis |
| Multiple Sclerosis |
| Parkinson’s Disease |
| Seizure Disorder |
| Spinal Cord Injury |
Ophthalmic
Care plans focusing on eye disorders:
| Ophthalmic Care Plans |
|---|
| Cataracts |
| Glaucoma |
| Macular Degeneration |
Pediatric Nursing Care Plans
Nursing care plans (NCPs) tailored for pediatric conditions and diseases:
| Pediatric Nursing Care Plans |
|---|
| Child Abuse |
| Cleft Lip and Cleft Palate |
| Dying Child |
| Febrile Seizure |
| Hospitalized Child |
| Hydrocephalus |
| Otitis Media |
| Spina Bifida |
| Tonsillitis and Adenoiditis |
Reproductive
Care plans related to reproductive and sexual function disorders:
| Reproductive Care Plans |
|---|
| Cryptorchidism (Undescended Testes) |
| Hysterectomy |
| Hypospadias and Epispadias |
| Mastectomy |
| Menopause |
| Prostatectomy |
Respiratory
Care plans for respiratory system disorders:
| Respiratory Care Plans |
|---|
| Airway Clearance Therapy & Coughing |
| Apnea |
| Asthma UPDATED! |
| Aspiration Risk & Aspiration Pneumonia |
| Bronchiolitis UPDATED! |
| Bronchopulmonary Dysplasia (BPD) UPDATED! |
| Chronic Obstructive Pulmonary Disease (COPD) UPDATED! |
| Croup Syndrome |
| Cystic Fibrosis UPDATED! |
| Epiglottitis |
| Hemothorax and Pneumothorax UPDATED! |
| Ineffective Breathing Pattern (Dyspnea) |
| Impairment of Gas Exchange |
| Influenza (Flu) UPDATED! |
| Lung Cancer UPDATED! |
| Mechanical Ventilation |
| Near-Drowning |
| Pleural Effusion |
| Pneumonia |
| Pulmonary Embolism |
| Pulmonary Tuberculosis |
| Tracheostomy |
Urinary
Care plans related to the kidney and urinary system disorders:
| Urinary Care Plans |
|---|
| Acute Glomerulonephritis |
| Acute Renal Failure |
| Benign Prostatic Hyperplasia (BPH) |
| Chronic Renal Failure |
| Hemodialysis |
| Nephrotic Syndrome |
| Peritoneal Dialysis |
| Urolithiasis (Renal Calculi) |
| Urinary Elimination (Urinary Incontinence & Urinary Retention) |
| Urinary Tract Infection |
| Vesicoureteral Reflux (VUR) |
| Wilms Tumor (Nephroblastoma) |
Recommended Resources: Nursing Diagnosis Care Plan Books in PDF
To further enhance your understanding and skills in creating effective nursing care plans, consider exploring these recommended resources. These Nursing Diagnosis Care Plan Book Pdf options and physical books are invaluable tools for both students and practicing nurses.
Disclosure: Please note that the following are affiliate links from Amazon. Purchasing through these links supports our site at no extra cost to you. For more details, refer to our privacy policy.
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
Cover of Ackley and Ladwig’s Nursing Diagnosis Handbook, a highly recommended guide for evidence-based nursing care planning, essential for students and practicing nurses.
This handbook is highly favored for its evidence-based approach to nursing interventions. It employs a user-friendly, three-step system that guides you through patient assessment, nursing diagnosis formulation, and care plan development. It provides clear, step-by-step instructions on implementing care and evaluating patient outcomes, helping you to develop critical thinking and diagnostic reasoning skills. Many users appreciate its comprehensive coverage and practical application in real-world nursing scenarios. Look for potential PDF versions online for digital access.
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition)
Cover of the “Nursing Care Plans – Nursing Diagnosis & Intervention” 10th Edition book, a comprehensive resource for nursing students and professionals seeking detailed care plans and diagnostic guidance.
This resource features over two hundred care plans that are updated to reflect the latest evidence-based guidelines. The 10th edition includes new content on ICNP diagnoses, care plans for LGBTQ health issues, and expanded coverage on electrolytes and acid-base balance. It’s an excellent resource for nurses seeking current and comprehensive care planning information. Check for PDF editions to access this valuable content digitally.
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales
Cover of the Nurse’s Pocket Guide, a quick reference tool for nursing diagnoses, prioritized interventions, and rationales, ideal for on-the-go access and efficient care planning.
This quick-reference tool is essential for identifying accurate diagnoses and planning patient care efficiently. The 16th edition includes the most recent nursing diagnoses and interventions, with an alphabetized listing of nursing diagnoses covering more than 400 disorders. Its pocket-size format makes it ideal for quick consultations in clinical settings. Digital PDF versions might be available for electronic access.
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care
Cover of the Nursing Diagnosis Manual, a detailed guide for planning, individualizing, and documenting client care, offering comprehensive support for nursing practice and documentation.
This manual is designed to help nurses plan, individualize, and document care for over 800 diseases and disorders. It uniquely provides subjective and objective data for each diagnosis, sample clinical applications, prioritized actions/interventions with rationales, and dedicated documentation sections. It’s a thorough guide for ensuring comprehensive and well-documented patient care. Explore options for a PDF version for convenient digital use.
Cover of the All-in-One Nursing Care Planning Resource E-Book, a comprehensive digital resource covering medical-surgical, pediatric, maternity, and psychiatric-mental health nursing care plans.
This e-book is a comprehensive resource featuring over 100 care plans across medical-surgical, maternity/OB, pediatrics, and psychiatric and mental health nursing. It uses interprofessional “patient problems” to help familiarize you with effective patient communication. Being an e-book, it naturally offers a PDF format for easy digital access and portability.
These resources, whether in physical or PDF format, are essential for any nurse aiming to master the art and science of nursing care planning and nursing diagnosis. They provide the knowledge and tools necessary to deliver patient-centered, effective, and evidence-based care.