Systemic Lupus Erythematosus (SLE) is a chronic autoimmune condition where the body’s immune system mistakenly attacks its own tissues and organs. This can lead to widespread inflammation and damage in various parts of the body. While the exact cause of SLE remains unknown, a combination of genetic predisposition, hormonal influences, and environmental triggers are believed to play a role. In healthy individuals, the immune system produces antibodies to defend against foreign invaders. However, in SLE, this system malfunctions, producing autoantibodies that target the body’s own cells. These autoantibodies and antigens form immune complexes, which deposit in tissues, causing inflammation, tissue injury, and pain. SLE can range from mild, affecting primarily the skin and joints, to severe, impacting major organs like the kidneys, heart, lungs, blood vessels, nervous system, and brain.
There are distinct types of lupus. Discoid lupus primarily affects the skin, with systemic involvement being rare. Systemic lupus erythematosus is more prevalent and severe, potentially affecting any organ system. It is characterized by periods of flares and remissions. Drug-induced lupus, the third type, is triggered by certain medications such as hydralazine, procainamide, isoniazid, chlorpromazine, d-penicillamine, and some anti-seizure drugs. Symptoms usually resolve upon discontinuation of the causative medication.
Nursing Care Priorities for SLE
Nursing care for patients with Systemic Lupus Erythematosus (SLE) focuses on managing symptoms, minimizing flares, and improving quality of life. Key nursing priorities include:
- Comprehensive assessment to identify SLE signs and symptoms.
- Administering prescribed medications like corticosteroids and immunosuppressants to manage disease activity.
- Continuous monitoring of disease progression, including organ involvement and potential complications.
- Educating patients on medication adherence and potential side effects.
- Providing holistic support for symptom management and minimizing triggers.
Nursing Assessment for SLE
A thorough nursing assessment is crucial for identifying the specific needs of patients with SLE. This involves gathering both subjective and objective data.
Nursing Diagnoses for SLE
Based on a comprehensive assessment, nursing diagnoses are formulated to address the specific challenges presented by Systemic Lupus Erythematosus (SLE). These diagnoses are guided by the nurse’s clinical judgment and understanding of the patient’s individual condition. Nursing diagnoses provide a framework for organizing care and prioritizing patient needs. Here are examples of nursing diagnoses relevant to SLE:
Nursing Goals for SLE Patients
Nursing goals for individuals with SLE are patient-centered and aim to improve their overall well-being. These goals may include:
- Patient will verbalize effective coping strategies for managing hair loss.
- Patient will identify and utilize appropriate methods to manage scalp changes due to hair loss.
- Patient will maintain optimal skin integrity, as evidenced by the absence of new rashes or skin lesions.
- Patient will report pain and stiffness at a manageable level (e.g., less than 3-4 on a 0-10 pain scale).
- Patient will actively participate in a personalized pain management plan incorporating both pharmacological and non-pharmacological approaches.
- Patient will demonstrate the ability to perform self-care activities independently or with assistance as needed.
- Patient will verbalize a clear understanding of the SLE disease process and their treatment plan.
Nursing Interventions and Actions for SLE
Nursing interventions for Systemic Lupus Erythematosus (SLE) are tailored to address the specific nursing diagnoses and patient needs.
1. Enhancing Skin Integrity
Maintaining skin integrity is paramount in SLE care due to the frequent skin manifestations of the disease.
Nursing Actions:
- Assess skin integrity meticulously. Observe for oral and nasal lesions, and discoid lesions on the face and chest.
- Evaluate patient’s pain description related to skin issues. Pain assessment guides effective treatment.
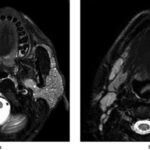
- Monitor for erythematous rashes, particularly the classic “butterfly” rash on the face. Note location and characteristics.
 Erythematous butterfly rash on the face of a patient with lupus
Erythematous butterfly rash on the face of a patient with lupus
- Assess for photosensitivity. Document any history of rash flares or disease exacerbation after sun exposure.
- Determine the impact of skin symptoms on lifestyle and body image. Understand the patient’s emotional response to skin changes.
- Promote adequate nutrition and hydration. Support skin health and wound healing through optimal intake.
- Educate on skin care: Advise gentle cleansing with warm water, moisturizing with unscented lotion, and using mild shampoo.
- Instruct to avoid harsh chemicals, hair dyes, and relaxers. These can exacerbate skin irritation.
- Recommend pressure-relieving devices. Prevent skin breakdown, especially over bony prominences.
For Skin Rashes:
- Advise protective eyewear, wide-brimmed hats, and umbrellas. Minimize sun exposure.
- Recommend high SPF sunscreen (SPF 15 or higher). Sunbathing is contraindicated.
- Educate on avoiding ultraviolet (UV) rays. Sunlight can trigger flares.
- Inform about specialized makeup. Suggest camouflage makeup to cover rashes and improve body image.
- Educate on hydroxychloroquine use. Explain its role in reducing inflammation and rash, onset of action (8-12 weeks), and the need for regular eye exams due to potential retinal toxicity. Also, discuss topical corticosteroids.
For Oral Ulcers:
- Advise avoiding spicy and citrusy foods. These can irritate oral ulcers.
- Instruct on keeping ulcers clean and dry. Apply dressings as needed to prevent infection and promote healing.
For Hair Loss:
- Educate that hair loss can occur during disease exacerbations. Scalp hair loss may be temporary and regrowth may occur during remission.
- Explain that certain medications (corticosteroids, immunosuppressants) can cause hair loss. Hair regrowth is expected as dosage decreases.
- Encourage exploration of strategies to manage hair loss. Suggest scarves, hats, or wigs to improve self-image.
2. Managing Acute Pain and Enhancing Comfort
Pain management is a crucial aspect of SLE nursing care due to joint pain and inflammation.
Nursing Actions:
- Assess pain characteristics. Evaluate joint pain, morning stiffness, and its relation to activity. Differentiate SLE-related stiffness from activity-related stiffness.
- Evaluate pain impact on function. Determine how pain affects interpersonal, social, and professional activities.
- Assess for joint inflammation signs. Monitor for warmth, redness, swelling, and reduced range of motion, noting that typical inflammation signs may be subtle in SLE.
- Review previous pain relief measures. Explore both pharmacological and non-pharmacological methods the patient has used.
- Encourage assistive devices for ambulation. Recommend crutches, walkers, or canes to reduce weight-bearing on painful joints.
- Promote anatomically correct positioning. Suggest a small pillow for the head and avoid knee gatch or pillows under knees to prevent contractures.
- Discourage prolonged inactivity. Encourage regular movement to prevent stiffness and muscle atrophy.
- Advise range-of-motion (ROM) exercises after warm showers or baths. Perform two repetitions per joint to improve mobility.
- Emphasize allowing sufficient time for activities. Joint stiffness can slow down task completion.
- Recommend 15-minute warm showers or baths upon waking. Warmth reduces stiffness and pain, avoiding excessive heat to prevent skin issues.
- Promote splint use as prescribed. Splints rest inflamed joints and reduce muscle spasms.
- Encourage non-pharmacological pain management. Suggest relaxation, distraction, and guided imagery.
- Suggest bed cradles. Keep bed covers off painful lower extremities.
- Administer anti-inflammatory medications as prescribed. Explain the importance of early morning dosing with a small snack.
- Administer non-opioid analgesics as needed. Opioids are less effective for inflammatory pain and carry habit-forming risks.
- Consult occupational therapy for splinting. Seek specialized expertise for optimal splinting.
3. Reducing Fatigue
Fatigue is a significant symptom in SLE, requiring comprehensive management.
Nursing Actions:
-
Assess fatigue characteristics. Evaluate timing, relation to activity, aggravating and alleviating factors to personalize energy management strategies.
-
Determine if psychological factors contribute to fatigue. Assess for stress and depression, common in chronic diseases.
-
Evaluate nighttime sleep patterns. Pain and discomfort can disrupt sleep.
-
Reinforce energy conservation principles:
- Adequate rest periods: Emphasize the need for increased rest.
- Pacing activities: Alternate activity with rest.
- Assistive devices: Promote proper use to conserve energy.
- Organization: Optimize environment and activity organization.
-
For sleep-related fatigue:
- Advise avoiding stimulants (caffeine) and stimulating activities before bed.
- Recommend warm baths or showers before bedtime.
- Promote anatomically correct sleep positioning.
- Encourage progressive muscle relaxation techniques.
- Advise frequent position changes during the night.
- Suggest gentle ROM exercises after warm showers or baths.
-
Administer nighttime analgesics or long-acting anti-inflammatory drugs as prescribed. Pain relief promotes rest and sleep.
4. Patient Education and Health Teaching
Empowering patients through education is crucial for self-management and improved outcomes in SLE.
Nursing Actions:
- Assess patient’s knowledge of SLE. Determine understanding of the disease, management, and potential complications.
- Educate about the disease process. Explain the unknown cause, chronicity, inflammation, fibrosis, remissions, exacerbations, and the goal of control vs. cure.
- Discuss common diagnostic tests. Explain the purpose of ANA, ESR, serum protein electrophoresis, rheumatoid factor, serum complement, and organ-specific assessments.
- Educate on drug therapy. Discuss potential side effects of steroids, immunosuppressants, and other SLE medications.
- Stress the importance of medication adherence. Emphasize not altering steroid doses or abruptly stopping medication due to adrenal insufficiency risk. Advocate for medical alert tags indicating steroid and immunosuppressant use.
- Instruct on monitoring for fever. Fever is a common SLE flare symptom, and accompanying chills, shaking, and diaphoresis should be reported. Caution about liver toxicity with aspirin use in SLE patients.
- Educate on lifestyle modifications to reduce flares:
- Balanced diet (fruits, grains, vegetables).
- Regular exercise.
- Sun avoidance.
- Adequate rest.
- Provide information on clinical trials. Discuss new therapies and research opportunities.
- Instruct on support groups and reputable online resources. Peer support can be beneficial.
5. Medication Administration and Pharmacologic Support
Pharmacological interventions are essential for managing SLE.
Nursing Actions:
- Administer antimalarials (chloroquine, hydroxychloroquine) as prescribed. Monitor for rare side effects and emphasize regular ophthalmologic exams.
- Administer corticosteroids as prescribed. Monitor for side effects like facial puffiness, buffalo hump, diabetes, osteoporosis, avascular necrosis, cataracts, and infection risk.
- Administer NSAIDs and COX-2 inhibitors as prescribed. Advise taking with food to avoid GI distress.
- Administer immunosuppressants (mycophenolate mofetil, cyclophosphamide, azathioprine) as prescribed. Monitor for infection risk, bone marrow suppression, nausea, vomiting, sterility, hemorrhagic cystitis, and cancer risk.
6. Monitoring Diagnostic and Laboratory Results
Regular monitoring of diagnostic tests is vital for assessing disease activity and treatment effectiveness.
Nursing Actions:
- Monitor Antinuclear Antibody (ANA) test results. Track ANA levels as a primary SLE screening test.
- Monitor Anti-Double-Stranded DNA (anti-dsDNA) Antibody test results. Monitor anti-dsDNA levels for diagnosis confirmation and disease activity.
- Monitor Anti-Smith (anti-Sm) Antibody test results. Assess anti-Sm levels for diagnostic aid.
- Monitor Complement Component Tests (C3, C4, CH50) results. Track complement levels to assess disease activity.
- Monitor Complete Blood Count (CBC) results. Observe for anemia, leukopenia, or thrombocytopenia.
- Monitor Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) results. Track inflammation levels.
- Monitor Kidney Function Tests results. Assess urine analysis, proteinuria, BUN, and creatinine for renal involvement.
- Monitor Imaging Studies (X-rays, ultrasound, CT scans) results. Evaluate organ involvement and complications.
- Monitor Biopsy results. Review tissue biopsies (e.g., kidney biopsy) for organ involvement confirmation.
7. Assessing and Monitoring for Potential Complications
Early detection and management of complications are crucial in SLE care.
Nursing Actions:
- Monitor for signs and symptoms of disease activity. Regularly assess for joint pain, rashes, fatigue, organ-specific symptoms, and changes in lab values.
- Monitor renal function. Assess urine output, urine analysis, and renal function tests to detect lupus nephritis.
- Assess skin condition regularly. Monitor for new rashes, lesions, or photosensitivity.
- Monitor medication adherence and side effects. Ensure patient understanding of medication regimens and assess for adverse reactions.
- Provide psychological and emotional support. Assess mental health and provide emotional support, offering referrals for counseling or support groups as needed.
Recommended Resources
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition)
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care