Assessment
A comprehensive nutritional assessment is fundamental in determining an individual’s nutritional status and identifying potential risks for nutritional imbalances. This process begins with a thorough review of the client’s medical history, followed by a detailed client interview, a physical examination, and an analysis of laboratory and diagnostic test results.
Subjective Assessment
Subjective assessment involves gathering information through client interviews, focusing on their typical eating habits and identifying any risk factors. This data is primarily obtained directly from the client or, secondarily, from family members or caregivers. While a review of medical charts can provide a significant amount of subjective data, it’s crucial to validate this information with the client or their family to ensure accuracy and account for any changes over time. Key subjective data points for a nutritional assessment include age, gender, history of illnesses or chronic conditions, surgical history, dietary intake (using methods like a 24-hour diet recall or food diary), food preferences, cultural dietary practices, typical meal and snack timings, food allergies, specialized diets, and details about food shopping and preparation habits.
Further insights into cultural dietary preferences and restrictions can be found in resources detailing common religious and spiritual practices.
A detailed subjective nutritional assessment is also invaluable for pinpointing risk factors for nutritional deficiencies or excesses, which is crucial for formulating an accurate Nutrition Nursing Diagnosis Nanda. For instance, a history of eating disorders like anorexia or bulimia indicates a heightened risk for vitamin, mineral, and electrolyte imbalances, as well as potential body image concerns. Swallowing difficulties can lead to inadequate intake, failing to meet metabolic demands. Similarly, the use of recreational drugs or alcohol can compromise nutrient intake and absorption. Conversely, the use of nutritional supplements may lead to excessive nutrient intake and potential toxicity. Recognizing these risk factors empowers nurses to proactively anticipate potential nutritional problems and address complications as they arise. Ideally, nurses can identify subtle indicators of impending or actual nutritional dysfunction, preventing more severe issues from developing and ensuring accurate nutrition nursing diagnosis nanda.
Objective Assessment
Objective assessment data is derived from the nurse’s direct observations during physical examinations, using techniques like inspection, auscultation, and palpation. Nutritional status should be a key consideration throughout the physical exam.
The physical examination begins with general observations of the client’s overall condition. A well-nourished individual typically exhibits normal skin color and hair texture for their ethnicity, healthy nails, a Body Mass Index (BMI) within the healthy range for their height, and appears energetic. These initial observations are important for a preliminary nutrition nursing diagnosis nanda.
Accurate measurement and documentation of height and weight are essential. For infants and children, these measurements are plotted on growth charts to determine percentile rankings within the United States, helping to track consistent growth trends.
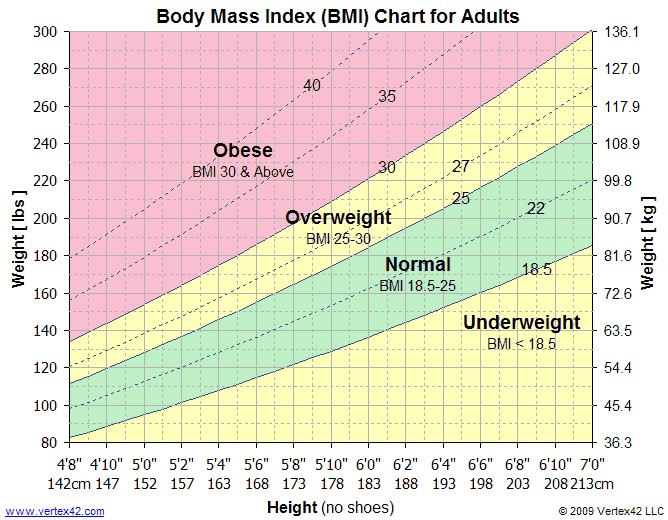
In adults, height and weight are often used to calculate the Body Mass Index (BMI). BMI can be calculated using the following formulas:
- BMI = weight (kilograms) / height (meters)²
- BMI = (weight (pounds) x 703) / height (inches)²
Alternatively, a BMI table can be used by plotting height on the horizontal axis and weight on the vertical axis, with the BMI indicated at the intersection. Figure 14.11 illustrates a BMI table for adults. BMI ranges are interpreted as follows:
- Less than 18.5: Underweight
- 18.5-24.9: Healthy weight range
- 25-29.9: Overweight
- 30 or greater: Obese
After completing both subjective and objective assessments, the collected data needs to be analyzed to identify both expected and unexpected findings. Table 14.3a compares expected versus unexpected assessment findings related to nutritional status, highlighting critical conditions (in bold) that necessitate immediate notification of a healthcare provider and are vital for accurate nutrition nursing diagnosis nanda.
Table 14.3a Expected Versus Unexpected Findings During Nutritional Assessment
| Assessment | Expected Findings | Unexpected Findings *Bolded items are critical conditions that require immediate health care provider notification. |
|---|---|---|
| General appearance | Energetic; normal skin, hair, and nails; and normal weight related to height | Lethargic, skin ulcerations, rashes, bruising, thinning or loss of hair, spooning of nails, obese, or underweight |
| Eyes | Normal vision and normal eye moisture | Impaired night vision or dry eyes |
| Mouth | Moist mucous membranes, intact oral mucosa, and intact smooth tongue | Dry/sticky mucous membranes, oral ulcerations, glossitis (swollen tongue), coughing while swallowing or inability to swallow, or swollen throat |
| Extremities/Integumentary | Normal skin, nontenting (good skin turgor) and supple texture | Tenting (poor skin turgor), dry skin, edema, or shiny skin |
| Neurological | Normal sensation and normal cognition | Numbness or tingling, tetany, dementia, or acute confusion |
| Cardiac | Normal heart tones, capillary refill | Bounding pulses, S3 heart tone, jugular venous distention, abnormal EKG tracing, or cardiac arrhythmias |
| Respiratory | Clear lung sounds throughout, normal respiratory rate, and no shortness of breath | Crackles in lung fields, pink frothy sputum, shortness of breath, or respiratory distress |
| Gastrointestinal | Normal stool quality and frequency for the client, bowel sounds present x 4 quadrants, and absence of nausea/vomiting | Constipation, diarrhea, nausea, or vomiting |
| Urinary | Clear urine, normal urine specific gravity, and urine output >30 mL/hr | Decreased urine output concentrated urine, or burning with urination**** |
| Weight | Normal BMI of 18.5-24.9, weight loss or gain of 0.5 to 1 pound per week is realistic, and | BMI 25, weight gain or loss of > 1kg over 24 hrs, or severe weight loss of >10% over 6 months |

Diagnostic and Lab Work
Diagnostic and laboratory results are crucial for providing detailed insights into a client’s nutritional status and should be interpreted alongside subjective and objective assessments to form a complete picture of their health. Common laboratory tests include hemoglobin (Hgb), hematocrit (HCT), white blood cell count (WBC), albumin, prealbumin, and transferrin levels. These tests are instrumental in supporting a precise nutrition nursing diagnosis nanda.
Anemia, characterized by low hemoglobin levels, is a condition that impairs oxygen transport throughout the body. While acute anemia can result from hemorrhage, it often stems from chronic deficiencies in iron, vitamin B12, or folate. Interventions such as iron supplements, vitamin B12 injections, folate supplements, and dietary adjustments to increase iron or folate intake can effectively raise hemoglobin levels.
Albumin and prealbumin are vital proteins in the bloodstream that maintain oncotic pressure, preventing fluid leakage from blood vessels into extravascular spaces. Low levels of these proteins are indicators of malnutrition, although they can also be influenced by conditions like liver and kidney failure, inflammation, and zinc deficiency. Albumin levels reflect long-term protein deficiency over several weeks, whereas prealbumin levels are more indicative of recent protein intake over the past few weeks. Consequently, prealbumin is frequently used to monitor the efficacy of parenteral nutrition therapy.
Transferrin, another crucial protein, is essential for iron transport on red blood cells. Transferrin levels typically increase in iron deficiency anemia but decrease in cases of renal or liver failure and infection. These lab values are essential data for determining the appropriate nutrition nursing diagnosis nanda.
Muscle wasting due to malnutrition can be quantified by measuring 24-hour urine creatinine levels. When caloric intake is insufficient, the body initiates catabolism, breaking down its own tissues for energy. This process releases blood urea nitrogen and creatinine as byproducts. Measuring these levels in a 24-hour urine collection helps assess the degree of catabolism occurring and is relevant to nutrition nursing diagnosis nanda related to malnutrition.
White blood cell counts tend to decrease with malnourishment, particularly in deficiencies of protein and vitamins C, D, E, and B-complex. Low WBC counts increase the risk of infection due to the critical role of white blood cells in a functioning immune system.
Table 14.3b provides a summary of selected lab values relevant to nutritional status and their nursing considerations. Always refer to your institution’s specific lab reference ranges when providing patient care to ensure accurate interpretation in the context of nutrition nursing diagnosis nanda.
Table 14.3b Selected Lab Values Associated with Nutritional Status
| Lab | Normal Range | Nursing Considerations***Bolded items are critical conditions and require immediate health care provider notification.** |
|---|---|---|
| Hemoglobin (Hgb) | Females: 12 – 16 g/dL Males: 14 – 17.4 g/dL |
Hemoglobin measures the oxygen-carrying capacity of blood. Decreased levels occur due to hemorrhage or deficiencies in iron, folate, or B12. 10 – 14: mild anemia 6 – 10: moderate anemia* Less than 6: severe anemia* |
| Hematocrit (Hct) | 37 – 50% | Hematocrit is normally three times the client’s hemoglobin level during normal fluid status. Increased levels occur with dehydration, and decreased levels occur with fluid overload or hemorrhage. |
| White blood cells (WBC) | 5,000 – 10,000 mm³ | Increased levels occur due to infection. Decreased levels occur due to prolonged stress, poor nutrition, and vitamins C, D, and E and B-complex deficiencies. Less than 4000: at risk for infection or sepsis Greater than 11,000: infection present |
| Magnesium | 1.6 – 2.6 mEq/L | Decreased level with poor nutrition or alcohol abuse. Increased levels due to kidney dysfunction. Critical values can cause cardiac complications such as arrhythmias or asystole: Less than 1.2 mg/dL or greater than 4.9 mg/dL |
| Albumin | 3.4 – 5.4 g/dL | Increased with dehydration. Decreased level due to zinc deficiency, corticosteroid use, protein deficiency over several weeks, or conditions resulting in muscle wasting/muscle loss. |
| Prealbumin | 15 – 36 mg/dL | Increased levels with corticosteroid or contraceptive use. Decreased levels due to inflammation, poor immunity, protein depletion over a few weeks. |
| Transferrin | 250 – 450 mcg/dL | Increased levels due to dehydration and iron deficiency. Decreased levels due to anemia; vitamin B12, folate, and zinc deficiency; protein depletion; and conditions resulting in muscle wasting/muscle loss. |
| 24-hour urine creatinine | Males: 0.8 – 1.8 g/24 hrs Females: 0.6 – 1.6 g/24 hrs |
Increased levels with renal disease and muscle breakdown. Decreased levels with progressive malnutrition as muscles atrophy. |
Depending on a client’s medical condition and specific circumstances, various diagnostic tests might be ordered. For example, a swallow study is used for clients experiencing dysphagia. Abdominal X-rays can confirm feeding tube placement or identify excess gas or stool in the colon. Barium swallows, often used with CT scans, can detect intestinal blockages. These diagnostic tests provide further objective data that refines the nutrition nursing diagnosis nanda.
Life Span and Cultural Considerations
Newborns and Infants
The period from birth to age two is critical for growth and development. Nutrient-dense food choices are essential during this stage to support proper growth, development, and brain function, especially given the relatively small food intake compared to adults and the rapid growth rate unique to this developmental phase. Ideally, newborns up to six months old should be exclusively breastfed to enhance immunity, although vitamin D and iron supplementation may be necessary. For the first few postpartum days, breast milk contains colostrum, a protein-rich fluid high in immunoglobulin A (IgA) but lower in carbohydrates and fat than mature breast milk. Colostrum is vital for protecting newborns from infections and establishing healthy gut bacteria. As breast milk matures after a few days, protein and IgA levels decrease, while carbohydrate and fat content increases. Human donor milk, sourced from accredited milk banks and pasteurized, can be used when breastfeeding is not possible. These factors are important to consider when assessing nutritional needs across the lifespan and formulating a nutrition nursing diagnosis nanda for infants.
For infants who cannot be breastfed or receive donor milk, iron-fortified commercial infant formula should be the exclusive source of nutrition until at least six months of age. Homemade or non-FDA-approved formulas, including toddler formulas, are not recommended due to their potential failure to meet infants’ high nutritional demands. Infants exclusively formula-fed typically do not require vitamin D supplementation.
Around six months, infants should gradually be introduced to nutrient-dense complementary foods that are developmentally appropriate, one at a time, to monitor for food sensitivities. This diversifies their diet, provides additional nutrients, and exposes them to different flavors and textures. Research suggests that early introduction to allergenic foods, like peanut butter before age one, can reduce the risk of developing allergies later in life. Honey and unpasteurized foods and drinks should be strictly avoided before age one to prevent botulism and other infections due to immature gut immunity. Cow’s milk, fortified soy drinks, and fruit or vegetable juices should also be avoided before the first year. These dietary guidelines are crucial when providing nutritional counseling and developing a nutrition nursing diagnosis nanda for this age group.
Children and Adolescents
Growth remains rapid from ages one to five, necessitating adequate nutrition to meet growth and metabolic demands. While caloric and nutritional requirements increase with age, dietary quality often declines. Younger children rely on adults for food choices, while older children and adolescents increasingly make independent food decisions, sometimes leading to less nutritious choices. Socioeconomic factors like poverty can also negatively impact nutrition in this age group. School lunch and breakfast programs play a vital role in mitigating poverty’s effects by providing nutritionally balanced meals at low or no cost. Understanding these influences is essential for creating effective nutrition nursing diagnosis nanda for children and adolescents.
Establishing healthy eating habits during childhood and adolescence is key to preventing obesity, cardiovascular disease, diabetes mellitus, and other chronic diseases in later life. Offering a variety of foods prepared in diverse ways can encourage children to accept and enjoy a wider range of foods. Picky eating is common; involving children in food selection and preparation can improve their acceptance of different foods.
Adults
Adulthood, spanning ages 19 to 59, often sees the consequences of poor nutritional habits established earlier in life. Changing these ingrained habits can be challenging due to food preferences and lack of nutritional knowledge. Metabolic rate and caloric needs decrease with age. Women generally require fewer calories than men, except during pregnancy and breastfeeding, when nutritional needs increase. Without balanced diet and physical activity, weight gain can occur, leading to obesity and chronic diseases. Over half of Americans face diet-related chronic conditions, highlighting the importance of nutritional awareness and intervention, which starts with accurate nutrition nursing diagnosis nanda.
Educating adults about healthy diets, including appropriate calorie, saturated fat, sugar, and sodium intakes, is crucial. A significant majority in the US exceed recommended intakes of saturated fat and sodium, while most do not consume enough dietary fiber, fruits, vegetables, and whole grains, contributing to chronic diseases.
Alcohol consumption can also undermine healthy eating. Chronic alcohol abuse impairs vitamin and mineral absorption, leading to general malnutrition. Alcohol intake should be limited to one drink per day for women and two for men, or avoided entirely by pregnant or breastfeeding women, individuals under 21, those with chemical dependencies, or underlying health conditions like diabetes. These lifestyle and dietary factors are critical components of a comprehensive nutritional assessment that informs the nutrition nursing diagnosis nanda for adults.
Pregnancy and Lactation
A balanced, healthy diet is vital during pregnancy and lactation to prevent complications for both mother and child. Nutritional requirements, including calories, vitamins, and minerals, increase during these periods. Increased caloric intake should come from nutrient-dense foods, not from calorie-dense, high-fat, high-sugar options. Prenatal vitamins and mineral supplements, along with a nutrient-rich diet, are often recommended to ensure adequate folic acid, iron, iodine, choline, and vitamin D intake. Folic acid is crucial in preventing neural tube defects in early pregnancy. Iron needs increase to support fetal development and prevent maternal anemia. Iodine and choline are essential for fetal neurocognitive development. These specific nutritional needs during pregnancy and lactation must be carefully considered when formulating a nutrition nursing diagnosis nanda for pregnant and breastfeeding women.
Older Adults
Older adults, aged 65 and above, are more susceptible to chronic illnesses and diseases. While their calorie needs are lower than younger adults due to decreased activity, metabolic rates, and muscle mass, their nutrient needs remain high. Chronic diseases and medications can further impair nutrient absorption. Protein and vitamin B12 deficiencies are common in older adults; protein is necessary to prevent muscle loss, and vitamin B12 absorption decreases with age and certain medications. Dehydration is also a concern as the sensation of thirst diminishes with age, and some older adults may restrict fluids due to bladder issues. Loneliness, chewing and swallowing difficulties, and poverty can also reduce dietary intake. Community programs like Meals on Wheels and senior centers can provide both socialization and balanced meals. Recognizing these age-related nutritional challenges is crucial for accurate nutrition nursing diagnosis nanda in older adults.
The Mini-Nutritional Assessment Short-Form is a valuable tool for screening older adults for malnutrition risk.
Download the Mini-Nutritional Assessment Short-Form from The Hartford Institute for Geriatric Nursing.
Diagnosis
Following a thorough assessment, data analysis, and clustering of relevant information, nursing diagnoses are selected based on defining characteristics. When developing a care plan, it is essential to consult current nursing care planning resources for the most up-to-date NANDA-I approved nursing diagnoses and interventions related to nutritional imbalances. This step is crucial in applying nutrition nursing diagnosis nanda effectively.
Examples of NANDA-I nursing diagnoses related to nutrition include:
Imbalanced Nutrition: Less than Body Requirements
Overweight
Obesity
Risk for Overweight
Readiness for Enhanced Nutrition
Impaired Swallowing
Table 14.3c provides detailed information about the diagnosis Imbalanced Nutrition: Less than Body Requirements, a key example of nutrition nursing diagnosis nanda.
Table 14.3c Sample NANDA-I Nursing Diagnosis Related to Nutrition
| NANDA-I Diagnosis | Definition | Selected Defining Characteristics |
|---|---|---|
| Imbalanced Nutrition: Less than Body Requirements | Intake of nutrients insufficient to meet metabolic needs. | Abdominal cramping Abdominal pain Body weight below ideal weight range for age and gender Diarrhea Food intake less than recommended daily allowance (RDA) Hyperactive bowel sounds Lethargy Pale mucous membranes Weight loss with adequate food intake |
A sample nursing diagnosis in PES (Problem, Etiology, Signs/Symptoms) format might be: “Imbalanced Nutrition: Less than Body Requirements related to insufficient dietary intake as evidenced by body weight 20% below ideal weight range and food intake less than recommended daily allowance.” This structured approach is central to nutrition nursing diagnosis nanda.
Outcome Identification
Goals for clients with nutritional alterations are determined by the specific nutrition nursing diagnosis nanda and the individual client’s situation. Generally, goals aim to resolve the nutritional imbalance and are broadly stated. A general goal for nutritional imbalances could be: “The client will achieve and maintain a weight within the normal range for their height and age.”
Outcome criteria need to be Specific, Measurable, Achievable, Realistic, and Time-oriented (SMART). A SMART goal example is: “By discharge, the client will identify three dietary modifications to align with USDA MyPlate guidelines to support their long-term health goals.” These outcomes provide measurable targets for evaluating the effectiveness of the nutrition nursing diagnosis nanda and subsequent interventions.
Planning Interventions
Once SMART outcome criteria are tailored to the client, nursing interventions are chosen to help achieve these outcomes. Interventions must be specific to the identified nutritional imbalance and sensitive to the client’s cultural and religious beliefs. The following outlines selected interventions related to nutrition therapy, essential components of implementing a care plan based on nutrition nursing diagnosis nanda.
Nutrition Therapy
- Identify nutritional risks
- Monitor food and fluid intake and calculate daily caloric intake as needed.
- Assess the appropriateness of the prescribed diet in meeting daily nutritional needs.
- Implement the prescribed calorie and nutrient intake to meet requirements.
- Determine food preferences, considering cultural and religious factors.
- Offer nutritional supplements as appropriate.
- Provide mealtime assistance to support dietary intake.
- Determine the necessity for enteral or parenteral nutrition.
- Manage enteral feeding or parenteral nutrition as indicated.
- Create a pleasant and relaxing mealtime environment.
- Present food attractively, considering color, texture, and variety.
- Encourage social mealtimes when appropriate.
- Promote adequate dental and mouth care.
- Assist the client to a sitting position before eating or feeding.
- Monitor laboratory values as needed.
- Educate the client and family about nutrition and prescribed diets.
- Refer to dietitians for detailed teaching and planning.
- Provide written dietary guidelines.
- Review medications and adjust if possible to minimize adverse nutritional effects.
- Encourage physical activity to maintain or improve muscle mass and function.
Clients may require special diets due to medical conditions or nutritional status. Table 14.3d lists commonly prescribed special diets, which are crucial in the planning phase following a nutrition nursing diagnosis nanda.
Table 14.3d Commonly Prescribed Special Diets
| Diet | Description | Example | Indication |
|---|---|---|---|
| NPO | Nothing by mouth–no food or drink allowed *Note: Oral care is very important during NPO status. | Oral care only | Before and after surgery or procedures, when peristalsis is absent, or during severe nausea or vomiting episodes, or for changes in mental status |
| Clear liquids | Fluids or solids that are liquid at room temperature, without residue, clear, or see-through | Water, apple juice, clear soda, Jello, popsicles, and broth | After surgery when peristalsis is slow and diet is being advanced from NPO status |
| Full liquids | Fluids with residue | Creamed soups, pudding, milk, orange juice, and creamed cereals | Next step after clear liquids as diet is being advanced |
| Mechanical soft | Chopped, ground, pureed foods that break apart easily without a knife | Soft cheeses, cottage cheese, ground meat, broiled or baked fish, cooked vegetables, and fruit | Poor or absent dentition; dysphagia |
| Pureed | Spoon thick with consistency of baby food | Applesauce, pudding, mashed potatoes, pureed meats, vegetables, and fruit | Dysphagia |
| Restrictive | Depends on the disease process | Diabetic: controlled amount of carbohydrates Cardiac: low fat and no added salt Renal: low-sodium and low-potassium containing foods |
Diabetes mellitus Heart disease Renal failure or dialysis |
“Thickened liquids” are often prescribed for clients with dysphagia, with three common consistencies: nectar-thick, honey-thick, and pudding-thick. Nurses often use commercial thickeners to achieve the prescribed consistency.
Enteral Nutrition
Enteral nutrition is a method of feeding that delivers nutrients directly to the gastrointestinal tract, bypassing chewing and swallowing. It is used for clients with impaired chewing or swallowing or those with poor nutritional intake or malnutrition. Enteral nutrition is a critical intervention often determined by the nutrition nursing diagnosis nanda.
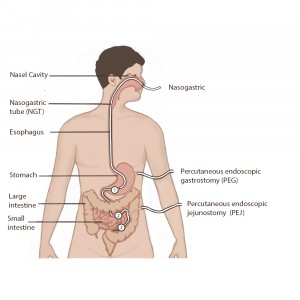
Enteral access can be achieved through nasogastric (NG) tubes, orogastric (OG) tubes, percutaneous endoscopic gastrostomy (PEG) tubes, or percutaneous endoscopic jejunostomy (PEJ) tubes. Figure 14.12 illustrates common enteral tube placements. NG tubes are inserted through the nose into the stomach, while OG tubes are inserted through the mouth, typically used for sedated or intubated clients. PEG tubes are surgically placed through the abdominal wall into the stomach, and PEJ tubes are placed into the jejunum, bypassing the stomach.
Nurses must adhere to safety protocols to prevent aspiration and dehydration during enteral nutrition administration. Tube placement verification is essential after insertion and before each feeding or medication administration to avoid pulmonary misadministration. Agency policies should be followed for placement checks. Current guidelines recommend verifying tube position every four hours and before administrations by measuring and comparing the external tube length to the documented length from X-ray verification. Older methods like auscultation of air insufflation or visual assessment of aspirate are no longer considered reliable.
To further prevent aspiration, nurses should maintain the head of the bed elevated at 30°-45°, use sedatives cautiously, regularly assess tube placement and external tube length, and monitor for gastrointestinal intolerance every four hours.
Gastric residual volume (GRV) measurement is often performed to assess tolerance to enteral feeding. Traditionally, GRVs of 200–500 mL triggered interventions like slowing or stopping feedings. However, current research suggests that stopping feedings for GRVs less than 500 mL, without other intolerance signs, is not recommended due to potential negative impacts on nutritional status. Routine GRV aspiration can also contribute to tube clogging. Agency policies should guide GRV monitoring and aspiration prevention strategies.
Clients receiving enteral nutrition should be monitored daily for signs of intolerance such as bloating, nausea, vomiting, diarrhea, cramping, and constipation. Room temperature formula administration can help alleviate cramping during bolus feedings. Providers should be notified of intolerance signs for potential formula or administration rate adjustments.
Electrolyte and blood glucose levels should also be monitored. Rapid carbohydrate absorption from tube feedings necessitates blood glucose monitoring, and elevated levels are typically managed with sliding scale insulin as prescribed.
Parenteral Nutrition
Parenteral nutrition provides nutrients intravenously, typically via a central line in the subclavian or internal jugular vein, for clients who cannot use enteral nutrition but require nutritional support. This method is considered when nutrition nursing diagnosis nanda indicates severe gastrointestinal dysfunction. Parenteral nutrition solutions contain glucose, amino acids, minerals, electrolytes, and vitamins, with lipids often administered separately. Total parenteral nutrition (TPN) provides complete nutritional support and is delivered via an IV pump.
Due to the high concentration of glucose, amino acids, and minerals, parenteral nutrition can irritate blood vessels, necessitating a large central vein for administration. Close monitoring of lab values is crucial to detect nutrient imbalances. Figure 14.13 shows a typical home parenteral nutrition setup with separate compartments for glucose, amino acids, and lipids, mixed just before use.
Parenteral nutrition is indicated when the gastrointestinal tract is non-functional, such as in paralytic ileus or post-bowel surgery, or in cases of severe malnutrition, burns, metastatic cancer, liver failure, or hyperemesis gravidarum.
Implementing Interventions
When implementing nutritional interventions based on nutrition nursing diagnosis nanda, it is essential to respect the client’s cultural and religious beliefs and food preferences.
For clients with nutritional deficits, pre-mealtime nursing interventions can enhance appetite. For example, managing pain or nausea with medication before meals, avoiding appetite-reducing procedures like dressing changes right before eating, and ensuring a pleasant, odor-free environment. If a meal is delayed and becomes cold, it should be reheated or replaced.
When assisting clients with meals, ensure hand hygiene and restroom use. Position clients comfortably in a chair or high Fowler’s position. Set up the meal tray and open containers as needed. Encourage self-feeding to promote independence. For visually impaired clients, use the clock method to describe food placement. When feeding, ask the client their preferred order of food and allow them to eat at their own pace, with time for chewing and swallowing between bites. Stop feeding and report any signs of swallowing difficulty, such as coughing or gagging, to the provider.
Evaluation
Evaluating the effectiveness of implemented interventions is critical to determine if they are appropriate and if adjustments are needed. Evaluation helps refine the care plan developed from the nutrition nursing diagnosis nanda. Table 14.3e lists assessment findings that indicate improvement in nutritional status.
Table 14.3e Evaluation of Alterations in Nutritional Status
| Imbalance | How Do We Know It Is Improved? |
|---|---|
| Imbalanced Nutrition: Less than Body Requirements | Stable or increasing weight; sufficient daily calories; well-balanced meal intake; improved energy, appearance of hair, nails, skin, or vision |
| Imbalanced Nutrition: More than Body Requirements | Stable or decreasing weight |
Definitions:
Body Mass Index (BMI): A measure of weight categories including underweight, normal weight, overweight, and obese taking height and weight into consideration.
Colostrum: A thick yellowish-white fluid rich in proteins and immunoglobulin A (IgA) and lower in carbohydrates and fat than mature breast milk secreted within the first 2-3 days after giving birth.
Lactation: Breast milk production.
Enteral nutrition: Liquid nutrition given through the gastrointestinal tract via a tube while bypassing chewing and swallowing.
Parenteral nutrition: An intravenous solution containing glucose, amino acids, minerals, electrolytes, and vitamins, along with supplemental lipids.