Understanding Nursing Diagnosis
A nursing diagnosis represents a critical clinical judgment. It focuses on a patient’s response to health conditions, life processes, or their vulnerability to such responses. This judgment is made for individuals, families, groups, or communities. Essentially, a nursing diagnosis serves as the foundation for selecting specific nursing interventions. These interventions are designed to achieve measurable outcomes for which nurses are accountable. Nursing diagnoses are not formed in isolation; they are meticulously developed using data collected during a thorough nursing assessment. This diagnosis empowers nurses to create personalized and effective care plans.
The Significance of Nursing Diagnosis
Nursing diagnoses serve several crucial purposes within healthcare:
- Enhancing Student Learning: For nursing students, the process of formulating nursing diagnoses is an invaluable educational tool. It sharpens problem-solving abilities and cultivates critical thinking skills essential for effective nursing practice.
- Prioritizing Care: Nursing diagnoses are instrumental in identifying immediate nursing priorities. They guide the direction of nursing interventions, ensuring that care is delivered strategically based on the most pressing patient needs.
- Meeting Quality Standards: Formulated nursing diagnoses contribute to establishing expected outcomes. This is vital for meeting the quality assurance requirements increasingly demanded by healthcare payers and regulatory bodies.
- Understanding Patient Responses: Nursing diagnoses offer a framework to understand how patients or groups react to both actual and potential health challenges and life events. Furthermore, they highlight available patient resources and strengths that can be leveraged to prevent or resolve health issues.
- Facilitating Communication: By providing a standardized language, nursing diagnoses enhance communication and foster mutual understanding among nursing professionals and the broader interdisciplinary healthcare team. This common language ensures clarity and consistency in patient care discussions.
- Evaluating Care Effectiveness: Nursing diagnoses establish a clear basis for evaluation. This allows healthcare providers to objectively determine if the nursing care provided was beneficial to the patient’s well-being and also cost-effective for the healthcare system.
Nursing Diagnosis vs. Medical Diagnosis vs. Collaborative Problems
It’s important to differentiate nursing diagnoses from related concepts. The term itself represents the second distinct phase in the nursing process, the “Diagnosis” phase within the ADPIE framework (Assess, Diagnose, Plan, Implement, Evaluate). Furthermore, “nursing diagnosis” is also the label assigned when nurses interpret collected patient data and categorize it appropriately.
For instance, during a patient assessment, a nurse might observe that a patient is experiencing anxiety, expresses fear, and has difficulty falling sleep. These observations are then translated into specific nursing diagnoses: Anxiety, Fear, and Disturbed Sleep Pattern, respectively. In this context, the nursing diagnosis is fundamentally rooted in the patient’s response to their medical condition. It is termed a ‘nursing diagnosis’ because it addresses areas where nurses have the autonomy and responsibility to act independently in managing the patient’s care related to a specific disease or condition. This encompasses physical, emotional, mental, and spiritual responses. Therefore, a nursing diagnosis prioritizes holistic patient care.
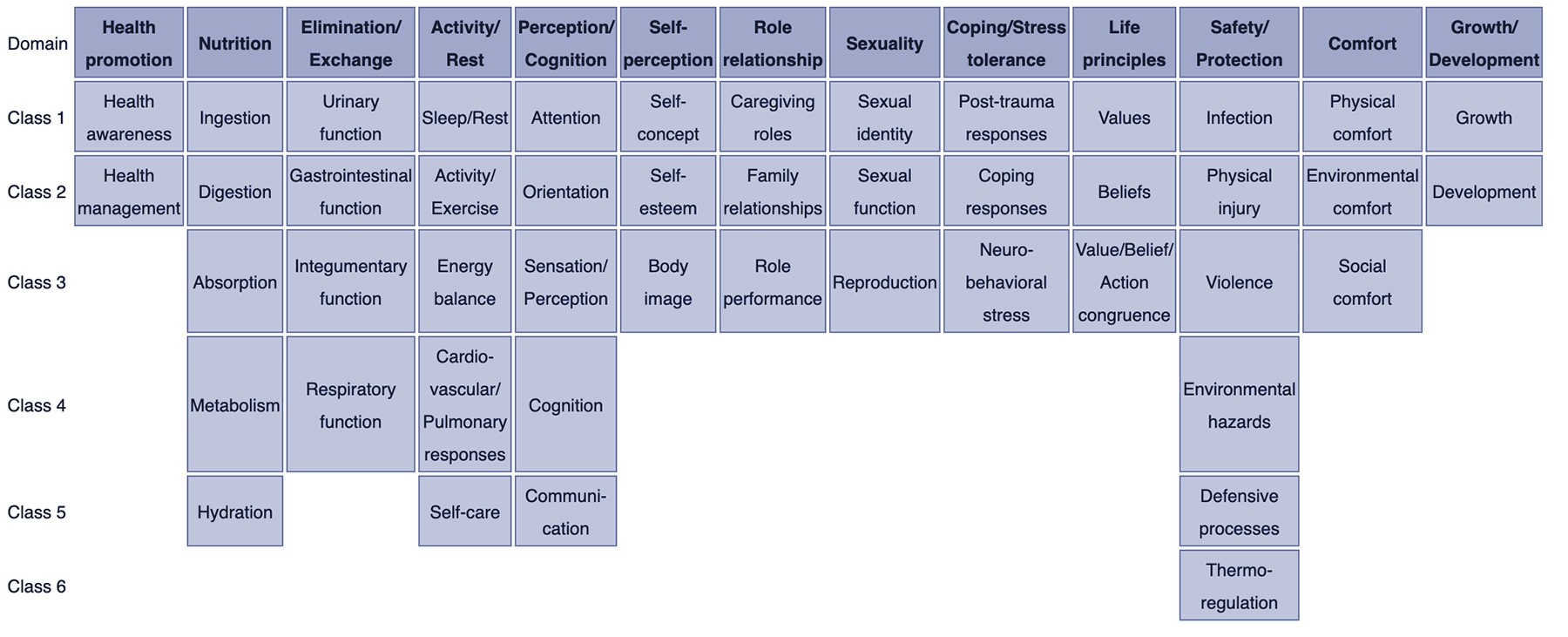
NURSING DIAGNOSIS TAXONOMY II. Taxonomy II for nursing diagnosis contains 13 domains and 47 classes. Image via: Wikipedia.com
In contrast, a medical diagnosis is the domain of physicians or advanced healthcare practitioners. It centers on identifying the disease, medical condition, or pathological state that only a physician can treat. Through their expertise and clinical judgment, physicians pinpoint the precise clinical entity that is the root cause of the illness. This medical diagnosis then guides the appropriate medication and medical interventions aimed at curing the disease. Examples of medical diagnoses include Diabetes Mellitus, Tuberculosis, Amputation, Hepatitis, and Chronic Kidney Disease. Medical diagnoses typically remain constant throughout the course of the illness. Nurses play a vital role in implementing the physician’s orders and executing prescribed medical treatments and therapies.
Collaborative problems represent potential complications that nurses manage through a combination of independent nursing actions and physician-prescribed interventions. These are health issues that necessitate both medical and nursing interventions. The nursing role in collaborative problems primarily involves continuous monitoring of the patient’s condition and proactive measures to prevent the development of potential complications arising from the medical condition.
As outlined above, the distinction between nursing diagnosis and medical diagnosis becomes clearer. Nursing diagnosis is patient-centered, focusing on the individual’s physiological and psychological responses to illness. Conversely, a medical diagnosis is disease-centered, concentrating on the specific illness or medical condition itself.
Classifying Nursing Diagnoses: Taxonomy II
How are nursing diagnoses organized and categorized? In 2002, Nursing Diagnosis Taxonomy II was adopted, building upon Dr. Mary Joy Gordon’s Functional Health Patterns assessment framework. Taxonomy II structures nursing diagnoses across three hierarchical levels: Domains (13 broad categories), Classes (47 more specific groupings within domains), and individual nursing diagnoses. Importantly, nursing diagnoses are no longer directly grouped by Gordon’s Functional Health Patterns. Instead, they are coded using seven axes: diagnostic concept, time, unit of care, age, health status, descriptor, and topology. Furthermore, diagnoses are now arranged alphabetically by their core concept, rather than the first word of the diagnosis title.
Here is a breakdown of the Domains and Classes within Taxonomy II:
- Domain 1. Health Promotion
- Class 1. Health Awareness
- Class 2. Health Management
- Domain 2. Nutrition
- Class 1. Ingestion
- Class 2. Digestion
- Class 3. Absorption
- Class 4. Metabolism
- Class 5. Hydration
- Domain 3. Elimination and Exchange
- Class 1. Urinary function
- Class 2. Gastrointestinal function
- Class 3. Integumentary function
- Class 4. Respiratory function
- Domain 4. Activity/Rest
- Class 1. Sleep/Rest
- Class 2. Activity/Exercise
- Class 3. Energy balance
- Class 4. Cardiovascular/Pulmonary responses
- Class 5. Self-care
- Domain 5. Perception/Cognition
- Class 1. Attention
- Class 2. Orientation
- Class 3. Sensation/Perception
- Class 4. Cognition
- Class 5. Communication
- Domain 6. Self-Perception
- Class 1. Self-concept
- Class 2. Self-esteem
- Class 3. Body image
- Domain 7. Role relationship
- Class 1. Caregiving roles
- Class 2. Family relationships
- Class 3. Role performance
- Domain 8. Sexuality
- Class 1. Sexual identity
- Class 2. Sexual function
- Class 3. Reproduction
- Domain 9. Coping/stress tolerance
- Class 1. Post-trauma responses
- Class 2. Coping responses
- Class 3. Neurobehavioral stress
- Domain 10. Life principles
- Class 1. Values
- Class 2. Beliefs
- Class 3. Value/Belief/Action congruence
- Domain 11. Safety/Protection
- Class 1. Infection
- Class 2. Physical injury
- Class 3. Violence
- Class 4. Environmental hazards
- Class 5. Defensive processes
- Class 6. Thermoregulation
- Domain 12. Comfort
- Class 1. Physical comfort
- Class 2. Environmental comfort
- Class 3. Social comfort
- Domain 13. Growth/Development
- Class 1. Growth
- Class 2. Development
The Nursing Process and Nursing Diagnosis
The nursing process is a systematic, five-stage approach to patient care: assessment, diagnosing, planning, implementation, and evaluation. Critical thinking is paramount at every stage of this process. Beyond merely understanding the definitions of nursing diagnoses, nurses cultivate a deep awareness of the defining characteristics and behaviors associated with each diagnosis. They also consider related factors that contribute to the chosen diagnoses and identify appropriate nursing interventions to effectively address them.
For a more in-depth exploration of the steps, significance, purposes, and characteristics of the nursing process, refer to “The Nursing Process: A Comprehensive Guide”.
Types of Nursing Diagnoses
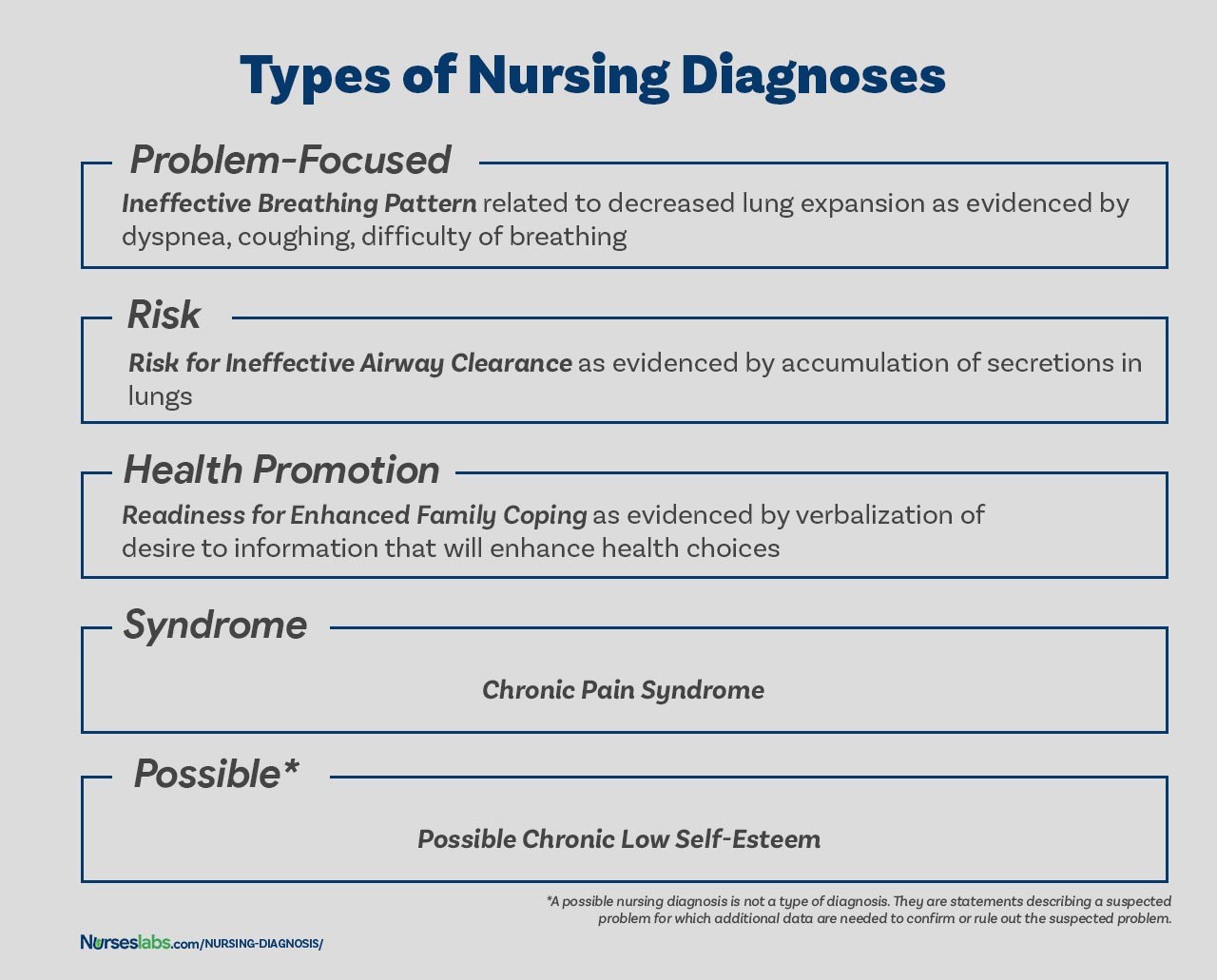
There are four primary types of nursing diagnoses: Problem-Focused (Actual), Risk, Health Promotion, and Syndrome. Understanding these categories is essential for accurate diagnosis and care planning.
TYPES OF NURSING DIAGNOSES. The four types of nursing diagnosis are Actual (Problem-Focused), Risk, Health Promotion, and Syndrome.
Problem-Focused Nursing Diagnosis
A problem-focused diagnosis, also known as an actual diagnosis, describes a current patient issue identified at the time of nursing assessment. These diagnoses are substantiated by the presence of observable signs and symptoms. It’s crucial to recognize that problem-focused diagnoses are not inherently more critical than risk diagnoses. In many clinical scenarios, a risk diagnosis may actually take precedence in terms of patient care priority.
Problem-focused nursing diagnoses are structured with three key components: (1) the nursing diagnosis label itself, (2) related factors contributing to the problem, and (3) defining characteristics – the signs and symptoms that evidence the problem. Examples of actual nursing diagnoses include:
Risk Nursing Diagnosis
Risk nursing diagnoses represent clinical judgments that a problem does not currently exist. However, the presence of specific risk factors indicates a significant likelihood that the problem will develop if nurses do not intervene proactively. A risk diagnosis is based on a patient’s current health status, past health history, and identified risk factors that elevate their susceptibility to experiencing a particular health issue. These diagnoses are integral to preventive nursing care, enabling early identification of potential problems and allowing nurses to implement strategies to prevent or minimize risk.
Risk diagnoses do not include etiological (related) factors in the same way as problem-focused diagnoses. Instead, the diagnosis highlights that the individual or group is more vulnerable to developing the problem compared to others in similar situations due to the identified risk factors. For example, an elderly patient with diabetes and vertigo who experiences difficulty walking and refuses assistance during ambulation could be appropriately assigned the risk diagnoses Risk for Injury or Risk for Falls.
IMPORTANT: In risk nursing diagnoses, the phrase “as evidenced by” connects the risk diagnosis label directly to the identified risk factors, rather than to defining characteristics (as there are none yet). Therefore, the components of a risk nursing diagnosis are:
- Risk diagnostic label, followed by “as evidenced by“
- Risk factors
Examples of risk nursing diagnoses are:
- Risk for Injury as evidenced by reduced cognitive awareness and use of sedative medications.
- Risk for Infection as evidenced by surgical wound, compromised immune system, and prolonged hospitalization.
- Risk for Falls as evidenced by muscle weakness, history of previous falls, impaired mobility, and use of assistive devices.
Health Promotion Diagnosis
Health promotion diagnoses, also known as wellness diagnoses, are clinical judgments concerning a patient’s motivation and desire to enhance their well-being and reach their full health potential. It articulates a patient’s readiness to engage in behaviors or activities that promote health and improve their quality of life. For instance, if a new mother expresses keen interest in learning optimal breastfeeding techniques, a nurse could formulate a health promotion diagnosis of “Readiness for Enhanced Breastfeeding.” This diagnosis then guides nursing interventions specifically designed to support the patient in learning and successfully implementing optimal breastfeeding practices.
Furthermore, health promotion diagnoses encompass an individual’s, family’s, or community’s transition from their current level of wellness to a higher state of well-being. Components of a health promotion diagnosis typically include only the diagnostic label itself, forming a one-part statement. However, for clarity, related factors can sometimes be added to further specify the context of the diagnosis. Examples of health promotion diagnoses include:
- Readiness for Enhanced Self-Care
- Readiness for Enhanced Nutrition
- Readiness for Enhanced Knowledge
- Readiness for Enhanced Parenting
- Readiness for Enhanced Family Processes
- Readiness for Enhanced Transition of Care
Readiness for Enhanced Transition of Care Nursing Diagnosis
This specific health promotion diagnosis, Readiness for Enhanced Transition of Care, is particularly relevant in today’s healthcare landscape, where continuity of care and seamless transitions between care settings are paramount. It signifies a patient’s willingness and proactive stance towards managing their health needs as they move from one care environment to another – for example, from hospital to home, or from acute care to long-term care.
This diagnosis acknowledges the patient’s expressed desire to actively participate in their transition plan, indicating they are prepared to learn about and implement necessary self-management strategies at home or in a new setting. It highlights their positive attitude and motivation to maintain or improve their health during and after the transition process.
Example Scenario:
Consider a patient recovering from a hip replacement surgery in the hospital. As discharge approaches, the nurse assesses the patient’s understanding of their post-operative care needs, medication regimen, and follow-up appointments. The patient actively asks questions, participates in discharge planning meetings, expresses confidence in managing their pain at home, and demonstrates a clear understanding of their rehabilitation exercises. In this case, the nurse might identify “Readiness for Enhanced Transition of Care” as a relevant nursing diagnosis.
Nursing Interventions for Readiness for Enhanced Transition of Care:
Nursing interventions for this diagnosis would focus on:
- Providing comprehensive discharge education: Covering medication management, wound care (if applicable), activity restrictions, diet, warning signs, and emergency contact information.
- Facilitating communication and coordination: Ensuring seamless communication between the hospital team, the patient, their family, and any receiving healthcare providers or community resources.
- Assessing and addressing barriers to transition: Identifying potential challenges the patient might face at home (e.g., lack of support, financial constraints, transportation issues) and proactively addressing them.
- Empowering patient self-management: Equipping the patient with the knowledge, skills, and resources necessary to confidently manage their health at home or in the new care setting.
- Arranging follow-up care: Scheduling necessary follow-up appointments with physicians, physical therapists, or other specialists.
By recognizing and addressing “Readiness for Enhanced Transition of Care,” nurses play a crucial role in ensuring smooth, safe, and patient-centered transitions, ultimately contributing to improved patient outcomes and reduced readmission rates.
Syndrome Diagnosis
A syndrome diagnosis is a clinical judgment that clusters together a group of actual or risk nursing diagnoses that are predictably likely to occur together due to a specific situation or event. Like health promotion diagnoses, syndrome diagnoses are typically written as a one-part statement, requiring only the diagnostic label. Examples of syndrome nursing diagnoses include:
- Rape Trauma Syndrome
- Disuse Syndrome
- Relocation Stress Syndrome
Possible Nursing Diagnosis
A possible nursing diagnosis is technically not a distinct type of diagnosis in the same category as actual, risk, health promotion, and syndrome diagnoses. Instead, “possible nursing diagnosis” is a statement used to describe a suspected problem that requires further data collection to either confirm or rule out. It serves as a communication tool among nurses, indicating that a potential diagnosis is being considered, but more data collection is needed to make a definitive determination. Examples include:
- Possible Spiritual Distress related to questioning of beliefs and values.
- Possible Situational Low Self-Esteem related to recent job loss.
Components of a Nursing Diagnosis
A comprehensive nursing diagnosis typically comprises three essential components: (1) the problem and its definition, (2) the etiology (for problem-focused diagnoses) or risk factors (for risk diagnoses), and (3) the defining characteristics (for problem-focused diagnoses) or risk factors (for risk diagnoses).
Problem and Definition
The problem statement, or diagnostic label, succinctly describes the patient’s health problem or response that warrants nursing intervention. A diagnostic label generally has two parts: a qualifier and the focus of the diagnosis. Qualifiers, also known as modifiers, are words added to some diagnostic labels to provide additional context, specificity, or limitation to the diagnostic statement. One-word nursing diagnoses (e.g., Anxiety, Constipation, Diarrhea, Nausea), where the qualifier and focus are inherent in the single term, are exceptions to this rule.
| Qualifier | Focus of the Diagnosis |
|---|---|
| Deficient | Fluid volume |
| Imbalanced | Nutrition: Less Than Body Requirements |
| Impaired | Gas Exchange |
| Ineffective | Tissue Perfusion |
| Risk for | Injury |
Etiology
The etiology, or related factors, component of a nursing diagnosis identifies the probable cause(s) or contributing factors to the health problem. These factors are the conditions or circumstances that are believed to be involved in the development of the problem. Identifying the etiology is crucial because it provides direction for targeted nursing therapy and allows nurses to individualize patient care. Nursing interventions should be strategically aimed at addressing the etiological factors to effectively resolve the underlying cause of the nursing diagnosis. Etiology is linked to the problem statement using the phrase “related to“. For example:
- Impaired Physical Mobility related to pain and stiffness.
- Deficient Knowledge related to lack of exposure to information.
Risk Factors
Risk factors are used in place of etiological factors for risk nursing diagnoses. Risk factors are elements that increase an individual’s or group’s vulnerability to developing an unhealthy condition. In a diagnostic statement, risk factors are written following the phrase “as evidenced by“.
- Risk for falls as evidenced by old age and use of walker.
- Risk for infection as evidenced by break in skin integrity.
Defining Characteristics
Defining characteristics are the clusters of observable signs and symptoms that strongly indicate the presence of a specific problem-focused nursing diagnosis. In actual nursing diagnoses, these defining characteristics are the patient’s identified signs and symptoms. For risk nursing diagnoses, signs and symptoms are not yet present; therefore, the risk factors that make the patient more susceptible to the problem serve as the evidence for the diagnosis. Defining characteristics are incorporated into the diagnostic statement using the phrases “as evidenced by” or “as manifested by“.
- Deficient Fluid Volume as evidenced by decreased urine output, dry mucous membranes, and poor skin turgor.
- Anxiety as manifested by restlessness, increased heart rate, and verbalization of worry.
The Diagnostic Process: A Step-by-Step Approach
The diagnostic process typically involves three distinct phases: (1) data analysis, (2) identification of the patient’s health problems, health risks, and strengths, and (3) formulation of diagnostic statements.
Analyzing Data
Data analysis involves a systematic comparison of patient data against established norms and standards, clustering related cues together, and identifying any gaps or inconsistencies in the data.
Identifying Health Problems, Risks, and Strengths
In this critical decision-making step, following data analysis, the nurse and the patient collaborate to identify problems that support potential actual, risk, and possible diagnoses. This involves differentiating between nursing diagnoses, medical diagnoses, and collaborative problems. Crucially, this stage also focuses on identifying the patient’s strengths, available resources, and coping abilities, which are essential for developing a holistic and patient-centered care plan.
Formulating Diagnostic Statements
The final step in the diagnostic process is the formulation of clear and concise diagnostic statements. The specific process for writing these statements is detailed in the next section.
Writing Effective Nursing Diagnoses
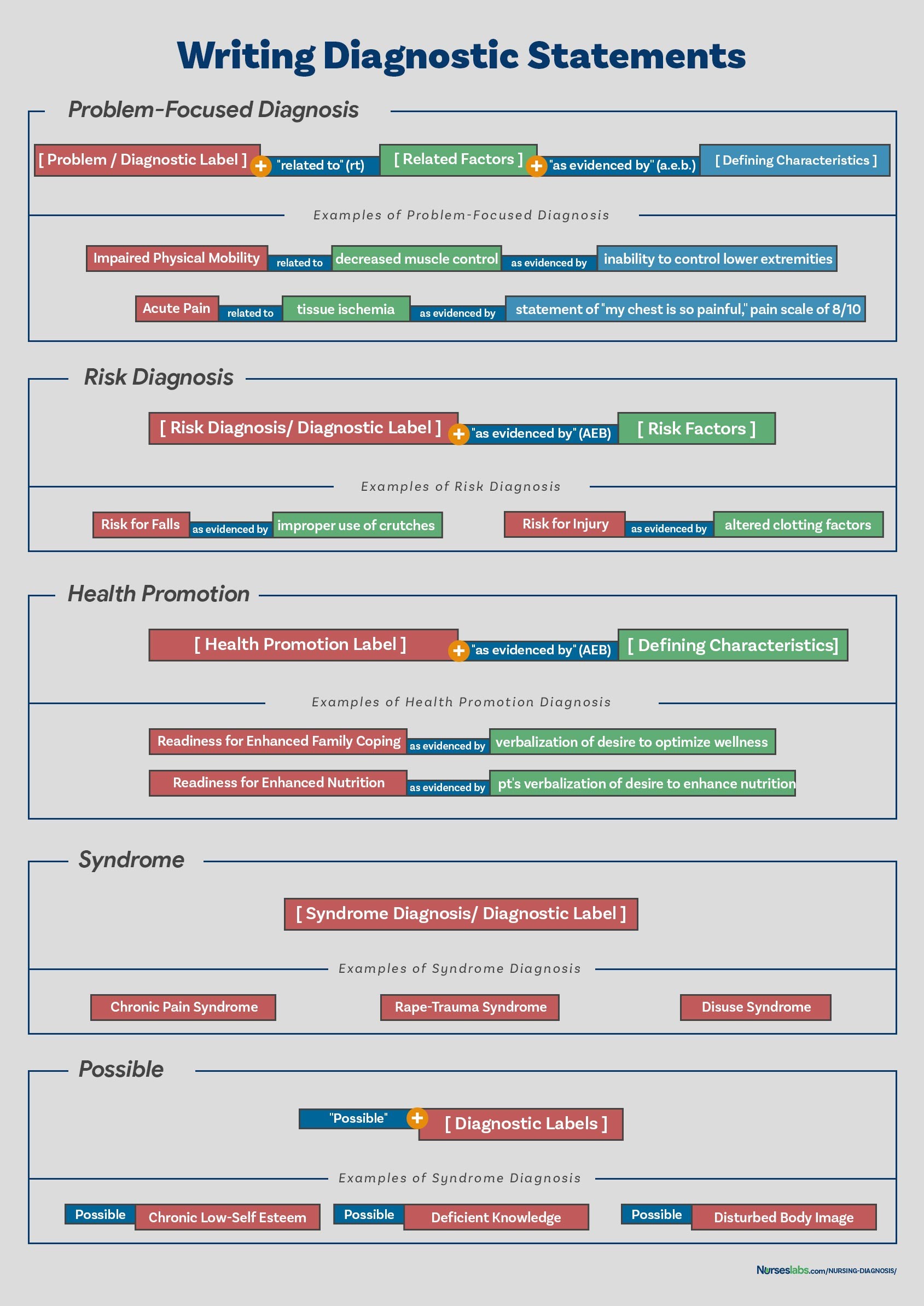
When writing nursing diagnostic statements, the goal is to accurately describe an individual’s health status and the contributing factors. It’s not always necessary to include all types of diagnostic indicators in every statement. The specific format for writing diagnostic statements will vary depending on the type of nursing diagnosis being formulated (as outlined below).
WRITING DIAGNOSTIC STATEMENTS. Your guide on how to write different nursing diagnostic statements.
The PES Format
Another widely used method for writing nursing diagnostic statements is the PES format. PES is an acronym that stands for:
- Problem (diagnostic label)
- Etiology (related factors)
- Signs/Symptoms (defining characteristics)
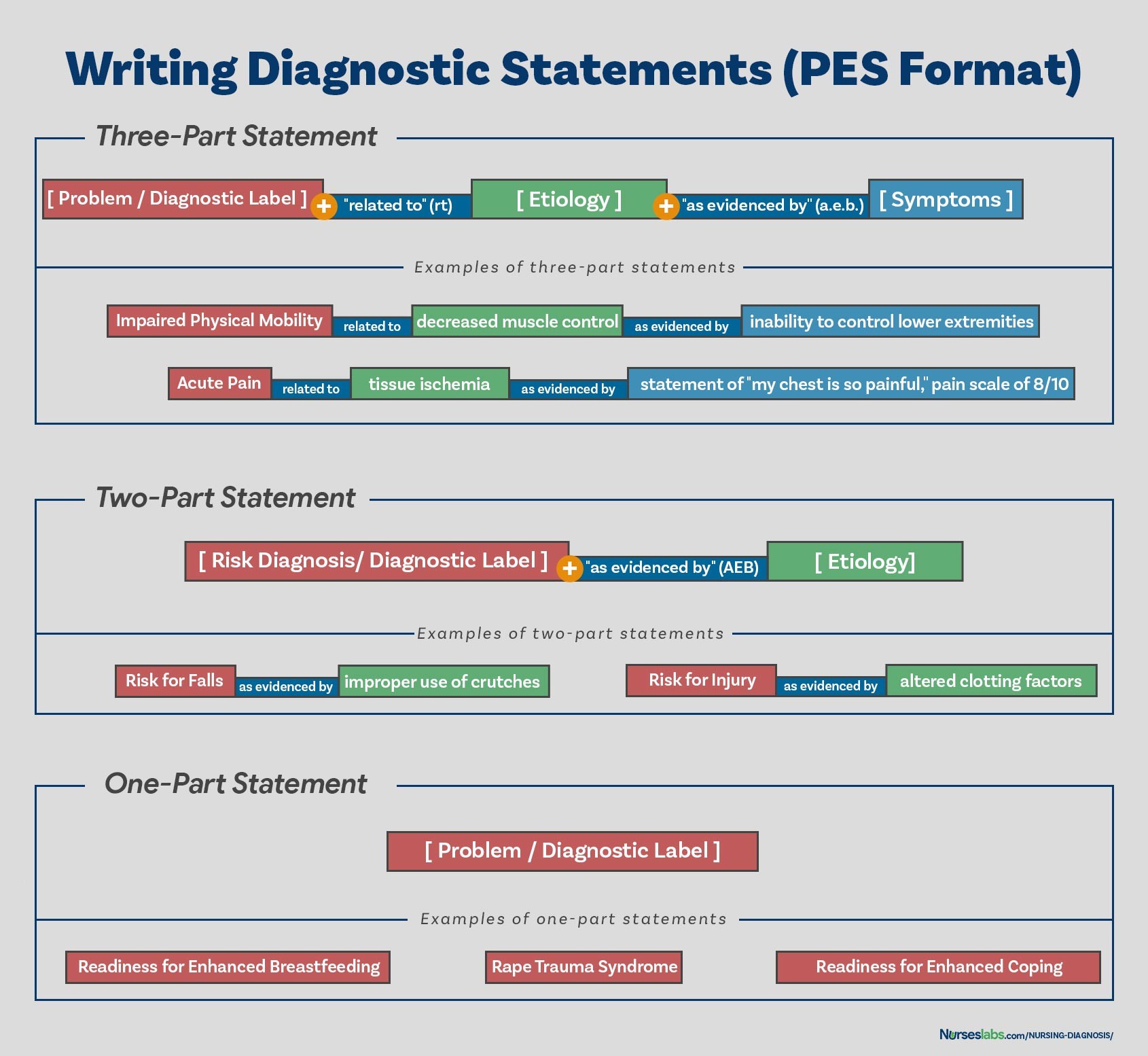
Diagnostic statements using the PES format can be structured as one-part, two-part, or three-part statements, depending on the type of diagnosis.
PES FORMAT. Writing nursing diagnoses using the PES format.
One-Part Nursing Diagnosis Statements
Health promotion nursing diagnoses are typically written as one-part statements. This is because the related factor is often inherent: the patient’s motivation to achieve a higher level of wellness. While related factors can be added to enhance clarity, they are not always necessary. Syndrome diagnoses also generally do not have related factors and are often written as one-part statements. Examples of one-part nursing diagnosis statements include:
- Readiness for enhanced coping
- Rape Trauma Syndrome
Two-Part Nursing Diagnosis Statements
Risk and possible nursing diagnoses commonly use two-part statements. The first part is the diagnostic label itself, and the second part provides the validation for a risk diagnosis (risk factors) or the reason for considering a possible diagnosis. It’s not appropriate to include a third part (signs and symptoms) for risk or possible diagnoses because, by definition, these are not yet present or confirmed. Examples of two-part nursing diagnosis statements include:
- Risk for Infection as evidenced by weakened immune system response.
- Risk for Injury as evidenced by unstable hemodynamic profile.
- Possible Spiritual Distress related to questioning of beliefs and values.
Three-part Nursing Diagnosis Statements
Actual or problem-focused nursing diagnoses are typically written as three-part statements, aligning with the PES format. These statements include: the diagnostic label (Problem), contributing factors (Etiology, linked by “related to”), and the supporting signs and symptoms (Signs/Symptoms, linked by “as evidenced by” or “as manifested by”). The three-part nursing diagnosis statement, therefore, fully encompasses the Problem, Etiology, and Signs and Symptoms – the PES format. Examples of three-part nursing diagnosis statements include:
- Acute Pain related to surgical incision as evidenced by patient report of pain at 7/10, guarding behavior, and increased heart rate.
- Ineffective Airway Clearance related to increased secretions as manifested by adventitious breath sounds, ineffective cough, and restlessness.
Variations on Basic Statement Formats
There are minor variations in how nursing diagnosis statements can be phrased, but the core components of Problem, Etiology, and Signs/Symptoms (or Risk Factors) remain consistent for each diagnosis type.
Nursing Diagnoses for Care Plans
This section provides a list or database of common nursing diagnosis examples that can be used to develop comprehensive nursing care plans.
See also: Nursing Care Plans (NCP): Ultimate Guide and List
Recommended Resources
The following are recommended resources, including nursing diagnosis and nursing care plan books, to further enhance your understanding and skills in this area.
Disclosure: Please note that affiliate links from Amazon are included below at no additional cost to you. We may earn a small commission from purchases made through these links. For more information, please refer to our privacy policy.
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care This handbook is highly recommended for its evidence-based approach to nursing interventions. It offers a user-friendly, three-step system to guide you through client assessment, nursing diagnosis, and care planning. The book provides step-by-step instructions on implementing care and evaluating outcomes, effectively building skills in diagnostic reasoning and critical thinking.
Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition) This resource includes over two hundred comprehensive care plans reflecting the most current evidence-based guidelines. New additions to this edition include ICNP diagnoses, specialized care plans addressing LGBTQ health issues, and expanded content on electrolytes and acid-base balance.
Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales This quick-reference tool provides essential information for accurately identifying diagnoses and efficiently planning patient care. The sixteenth edition features the latest nursing diagnoses and interventions, along with an alphabetized listing of nursing diagnoses covering over 400 disorders.
Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care This manual is invaluable for identifying interventions to effectively plan, personalize, and document care for over 800 diseases and disorders. Unique to this manual are subjectively and objectively organized diagnoses, sample clinical applications, prioritized action/interventions with rationales, dedicated documentation sections, and much more.
All-in-One Nursing Care Planning Resource – E-Book: Medical-Surgical, Pediatric, Maternity, and Psychiatric-Mental Health This comprehensive e-book includes over 100 care plans spanning medical-surgical, maternity/OB, pediatrics, and psychiatric and mental health nursing. The interprofessional “patient problems” focus helps familiarize users with patient-centered communication.
See also
Explore these other recommended resources on our site for further learning about nursing care plans:
References and Sources
The following references and sources were used in compiling this Nursing Diagnosis guide and are recommended for further reading and in-depth study.
- Berman, A., Snyder, S., & Frandsen, G. (2016). Kozier & Erb’s Fundamentals of Nursing: Concepts, process and practice. Boston, MA: Pearson.
- Edel, M. (1982). The nature of nursing diagnosis. In J. Carlson, C. Craft, & A. McGuire (Eds.), Nursing diagnosis (pp. 3-17). Philadelphia: Saunders.
- Fry, V. (1953). The Creative approach to nursing. AJN, 53(3), 301-302.
- Gordon, M. (1982). Nursing diagnosis: Process and application. New York: McGraw-Hill.
- Gordon, M. (2014). Manual of nursing diagnosis. Jones & Bartlett Publishers.
- Gebbie, K., & Lavin, M. (1975.) Classification of nursing diagnoses: Proceedings of the First National Conference. St. Louis, MO: Mosby.
- McManus, R. L. (1951). Assumption of functions in nursing. In Teachers College, Columbia University, Regional planning for nurses and nursing education. New York: Columbia University Press.
- Powers, P. (2002). A discourse analysis of nursing diagnosis. Qualitative health research, 12(7), 945-965.
