Introduction
Diabetic Kidney Disease (DKD), a frequent complication of diabetes mellitus, poses a significant threat due to its complexity and rapid progression towards end-stage renal disease. Traditional Chinese Medicine (TCM) offers a unique perspective on diagnosing and treating DKD, emphasizing individualized approaches based on syndrome differentiation. However, the intricate nature of TCM diagnosis, often reliant on expert experience and less on standardized guidelines, can present learning challenges, especially for new practitioners. Much of the valuable knowledge in TCM diagnosis and treatment remains embedded within medical records, creating “knowledge islands” that hinder efficient learning and knowledge dissemination. To bridge this gap and enhance the understanding and application of TCM in DKD, a structured, knowledge-driven approach is essential.
This article delves into the development and application of a comprehensive knowledge graph designed to systematize TCM diagnosis and treatment of DKD. This knowledge graph, built upon clinical guidelines, expert consensus, and real-world clinical data, serves as the foundation for creating a practical Tcm Diagnosis Chart – a visual and accessible tool to navigate the complexities of DKD diagnosis in TCM. By systematically organizing and mining TCM knowledge, this approach aims to make DKD diagnosis more transparent, facilitate knowledge sharing, and ultimately support clinicians in making informed decisions.
The power of knowledge graphs lies in their ability to represent knowledge semantically, connect disparate data points, and expand as new information becomes available. In medicine, and particularly in TCM, this technology offers a promising avenue for integrating and exploring the wealth of diagnostic and therapeutic knowledge. While much of the existing research on medical knowledge graphs focuses on technical advancements in algorithms and data processing, this study prioritizes addressing practical clinical challenges. We aim to overcome limitations seen in previous approaches by:
- Expanding Knowledge Sources: Moving beyond relying solely on guidelines and incorporating the rich data found in Electronic Medical Records (EMRs) to reflect the nuances of real-world clinical practice. Guidelines, while authoritative, may not capture the variability seen in individual patient presentations, influenced by factors like lifestyle, emotions, and genetics. EMRs, on the other hand, document the complete patient journey, offering a more holistic view.
- Refining Data Granularity: Addressing the issue of coarse data granularity often encountered when constructing medical knowledge graphs. By employing data mining techniques, we aim to extract finer details from clinical data, enriching the entities, attributes, and relationships within the graph, leading to more clinically relevant guidance.
Historically, studies exploring TCM diagnosis and treatment rules for DKD have often been limited in scope, focusing on narrow aspects of data analysis. This fragmented approach has hindered the development of a comprehensive TCM knowledge system for DKD. This paper addresses this gap by integrating DKD TCM diagnosis and treatment guidelines, consensus documents, and real-world medical records. The knowledge graph we constructed incorporates data mining insights, assigning weights and levels to relationships, paving the way for advanced knowledge reasoning. This TCM diagnosis chart, derived from the knowledge graph, is intended to make TCM diagnostic knowledge more accessible and user-friendly. Through relationship-based retrieval, we aim to uncover the implicit knowledge within TCM diagnosis and treatment of DKD, enabling continuous refinement and updating of this vital body of knowledge.
Alt Text: Diagram illustrating the two-dimensional relational mining process used to construct the TCM diagnosis chart for Diabetic Kidney Disease, showcasing relationships between disease stages, comorbidities, syndrome groups, symptoms, medical examinations, and Chinese herbs.
Materials and Methods
Research Process Overview
The primary goal of this research is to create an authoritative and practical TCM diagnosis chart for DKD, facilitating deeper knowledge discovery within this domain. The construction of the underlying knowledge graph followed an ontology-based approach, encompassing data preprocessing, analysis, ontology development, knowledge extraction, fusion, and storage. Once constructed, the graph enables knowledge visualization, retrieval, and discovery, ultimately informing the TCM diagnosis chart. A key distinction of this study is the initial data mining phase, which enhances the accuracy and clinical relevance of the knowledge graph and, consequently, the diagnosis chart. Furthermore, we explored implicit knowledge within the data through two-dimensional relationship analysis. The data sources feeding into the graph construction included:
- High-quality TCM diagnostic and treatment guidelines for DKD.
- Clinical medical records of DKD patients treated with TCM.
- Relational data derived from data mining techniques.
Alt Text: Flowchart outlining the methodology for developing the TCM diagnosis chart for Diabetic Kidney Disease, starting with data preprocessing and ontology construction, leading to knowledge visualization and retrieval.
Data Sources
The data for this study originated from two main sources:
- TCM Guidelines and Consensus: We incorporated authoritative guidelines, expert consensus documents, standards, and protocols related to TCM diagnosis and treatment of DKD. These included key documents such as the “Guidelines for the diagnosis and treatment of DKD combined with disease and syndrome (2022),” “TCM diagnosis and treatment plan for wasting-thirst kidney disease (diabetic kidney disease) (2017),” “TCM diagnosis and treatment standards for DKD (2011),” and “DKD diagnosis, syndrome differentiation, and efficacy evaluation standards (2007).”
- Clinical Medical Records: Effective inpatient medical records were collected from DKD patients hospitalized at Kaifeng Hospital of TCM between December 2018 and June 2021, totaling 1105 cases. These records contained crucial information on patient characteristics, symptom descriptions (including tongue, pulse, urine, and stool), treatment principles and methods, prescribed formulas, auxiliary examination results, and efficacy evaluations. The data encompassed Western medicine diagnoses, complications, comorbidities, TCM syndrome diagnoses, and prescribed medications.
Data Preprocessing
Data Screening
Data inclusion involved a two-stage screening process: primary database screening followed by manual secondary screening. The inclusion criteria were: 1) Confirmed diagnosis of type 2 DKD; 2) Age ≥ 18 years; 3) Complete essential information in patient data and medical records (including TCM and Western diagnoses, staging, syndrome diagnosis, chief complaint, symptoms, and at least two sets of laboratory examinations on admission and discharge); 4) Availability of efficacy evaluation information, indicating significant symptom improvement and indicator improvement or normalization post-treatment.
Efficacy Evaluation Analysis
Given the retrospective nature of the study, focusing on real-world TCM treatment data, efficacy evaluation was crucial to minimize bias and enhance the clinical applicability of the derived TCM diagnosis chart. We employed a combination of database and manual screening, referencing established “DKD diagnosis, syndrome differentiation, and efficacy evaluation standards (2007)” and “Studies about Specification of Syndrome Differentiation on Different Stages and Efficacy Evaluation Proposal for Diabetic Kidney Disease. (2017).” Expert feedback further informed the formulation of efficacy evaluation indicators for retrospective medical record data (Table 1). Ultimately, data from 1105 DKD patients treated with TCM met the inclusion criteria.
Table 1. Efficacy evaluation indicators of DKD.
| Evaluation indicators | Content of the evaluation description | Evaluation description |
|---|---|---|
| Main symptoms | edema、foamy urine、lack of strength、shortness of breath、dry mouth、thirst、constipation、numbness in limbs、positioning sting、soreness and weakness of the waist and knees, etc | improve、relieve、relief、vanish、ameliorate、inapparent、no recurrence、recovery. etc., |
| Urine-related indicators | mALB、24hUTP、UACR、UAER | decrease or return to normal |
| Blood-related indicators | GLU、HbA1c、SCr | decrease |



Alt Text: Table outlining the efficacy evaluation indicators used to assess patient data for the TCM diagnosis chart, including main symptoms, urine-related indicators, and blood-related indicators, with descriptions of positive evaluation outcomes.
Data Standardization
To address inconsistencies in terminology, conceptual ambiguities, and information clutter within the data, a data standardization process was implemented. This process aimed to normalize, organize, and improve data quality. Western medical diagnoses were standardized using the International Classification of Diseases-11 (ICD-11). Syndrome names were standardized according to “Clinic terminology of traditional Chinese medical diagnosis and treatment—Part 2: syndromes.” Syndrome element classification followed “syndrome differentiation of syndrome elements.” Symptom and sign data were standardized using “Standardized Terminology of Common Clinical Symptoms in TCM,” “Differential Diagnosis of Symptoms in TCM,” and “Terminology of TCM.” Therapeutic method specifications were derived from “Clinic terminology of traditional Chinese medical diagnosis and treatment—Part 3: therapeutic methods.” Finally, herbal medicine names were standardized using “the Pharmacopoeia of the People’s Republic of China (2020 edition).” Data standardization techniques included categorizing terms, unifying synonyms, filling in referential terms, and simplifying redundant terms (Table 2).
Table 2. Example of data standardization.
| Number | Standardized methods | Original terminology | Standardized terminology |
|---|---|---|---|
| 1 | Categorize to superior terms | Grade III hypertension, Hypertension Grade 3 (high risk) | Hypertension |
| 2 | Harmonization of synonymous terms | Xianlingpi, Epimedium | Epimedium |
| 3 | Normalization of the expression of irregular terms | Syndrome of intense exuberant fire toxin | Syndrome of intense exuberant heat toxin |
| 4 | Filling of pronouns | Numbness and tingling in both lower limbs | Numbness in the lower limbs, tingling in the lower limbs |
| 5 | Simplification of redundant terms | Itching of both feet | Itchy feet |
Alt Text: Table providing examples of data standardization methods applied to the TCM diagnosis chart project, showing original terminologies and their standardized counterparts across various categories.
Data Analysis
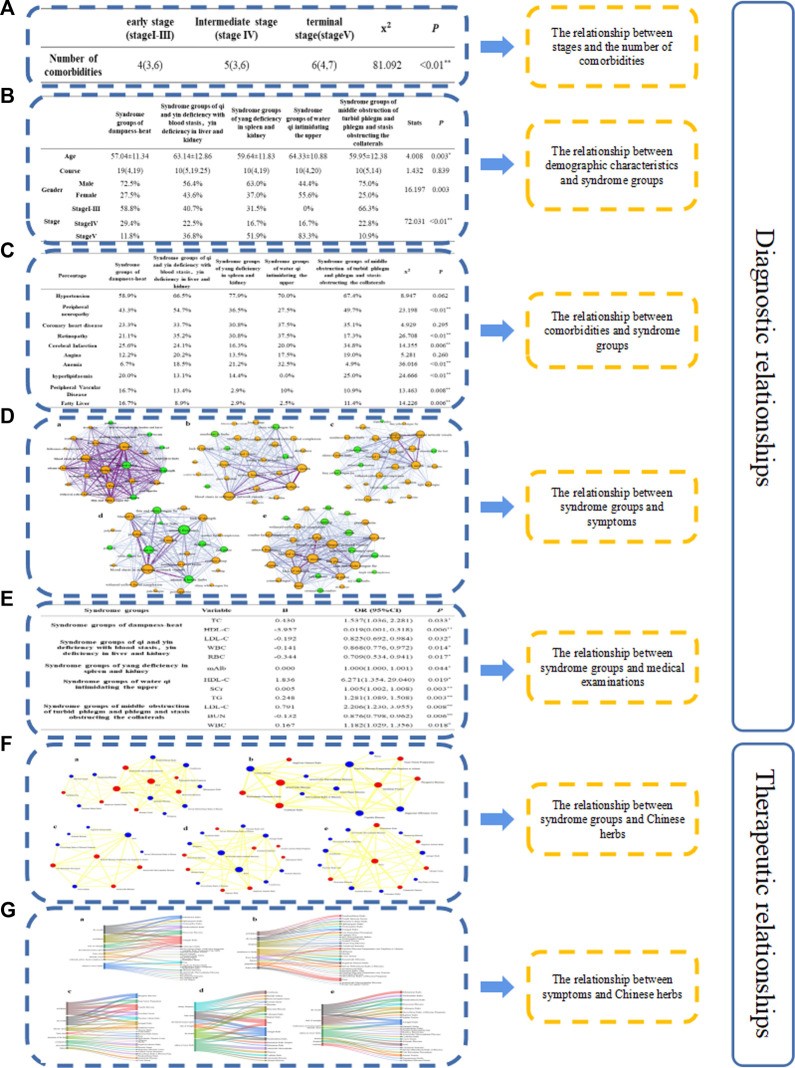
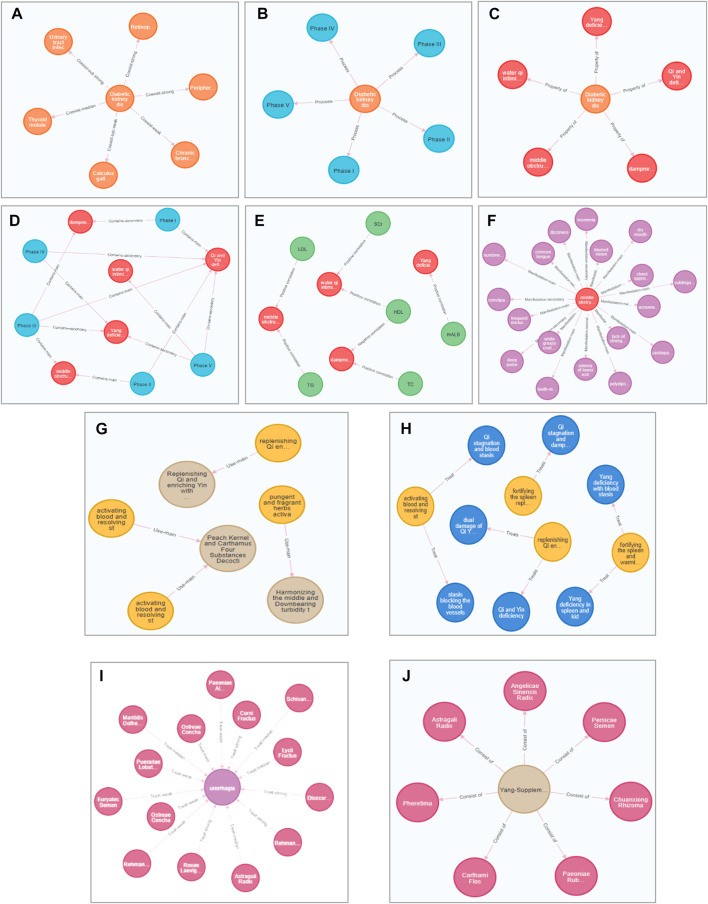
To achieve fine-grained entities and relationships for the TCM diagnosis chart and comprehensively represent TCM diagnostic knowledge, we conducted two-dimensional correlation knowledge mining from perspectives including “stage-number of comorbidities,” “comorbidity-syndrome groups,” “demographic characteristics-syndrome,” “syndrome groups-typical symptom,” “syndrome groups -medical examination,” “syndrome groups-Chinese herb,” and “symptom-Chinese herb” (Figure 2). Based on frequency distribution, relationships were weighted and assigned hierarchical levels. This relational mining enriched the data within the knowledge graph, providing a foundation for knowledge organization and discovery. This process yielded 79 correlations, associations, and treatment relationships (Table 3).
Table 3. Relationships from data mining.
| Number | Relationships | Type of relationships | Number of relationships |
|---|---|---|---|
| 1 | Stage-Number of comorbidities | correlation | 1 |
| 2 | Comorbidities-Syndrome groups | correlation | 7 |
| 3 | demographic characteristics-syndrome groups | correlation | 3 |
| 4 | syndrome groups- typical symptoms | contain | 5 |
| 5 | syndrome groups- medical examinations | correlation | 12 |
| 6 | syndrome groups-Chinese herbs (core prescriptions) | treat | 5 |
| 7 | Symptoms-Chinese herbs | treat | 38 |
Alt Text: Table listing the relationships derived from data mining for the TCM diagnosis chart project, categorizing them by type and quantifying the number of relationships identified in each category.
Ontology Construction
The DKD TCM diagnosis and treatment knowledge graph, which underpins the TCM diagnosis chart, consists of a pattern layer (ontology) and a data layer. The pattern layer defines the high-level structure, while the data layer contains specific diagnosis and treatment instances. Ontology construction aimed to capture and represent domain knowledge, establish shared understanding, define terms, and clarify relationships across formal pattern levels. We employed both top-down and bottom-up approaches. The top-down method defined a schema layer based on logical relationships and knowledge hierarchy, mapping data entities to it. The bottom-up approach extracted entities and attributes from data sources, consolidating them and refining the schema layer for iterative updates. This combined approach leveraged the professionalism of the top-down method and the practicality of the bottom-up method, crucial for the medical domain.
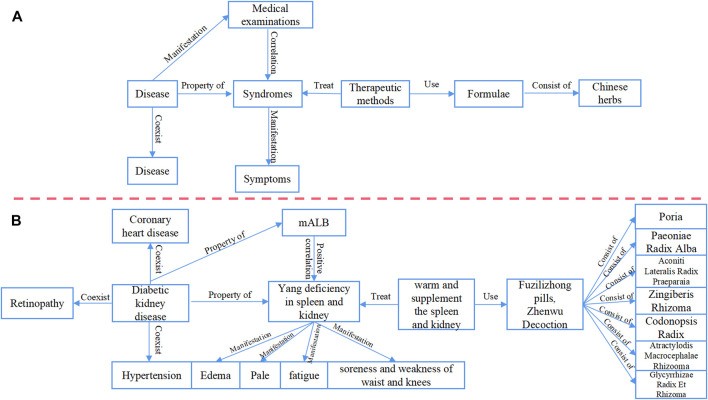
During data screening, standardization, and analysis, initial organization and standardization of DKD TCM diagnosis and treatment knowledge was performed. We utilized the Chinese Medicine Language System (TCMLS) for concept and semantic relation definition to build the ontology layer collaboratively. The data layer aimed to systematically categorize and explore DKD TCM diagnosis and treatment knowledge by mapping information into concepts and relationships using “entity-relationship-entity” and “entity-attribute-attribute value” triples (Figure 3).
Alt Text: Diagram illustrating the logical framework of the pattern and data layers within the TCM diagnosis chart’s knowledge graph, highlighting the structure of the ontology and data instances.
Knowledge Extraction
Data sources included unstructured guidelines and consensus documents, alongside semi-structured and structured clinical records. Given the complexity of TCM diagnostic data and the need for accuracy in the TCM diagnosis chart, we adopted a manual, interactive knowledge extraction approach. Two TCM practitioners manually extracted entities, relationships, and attributes, organizing them as triplets. Disagreements were resolved by a third senior TCM practitioner. This process focused on concepts and their relationships as the extraction framework, considering the hierarchical and weighted relationships derived from data mining.
Knowledge Storage
The Neo4j graph database was used for knowledge storage. Neo4j, a high-performance NoSQL graph database, utilizes nodes, edges, and attributes to store graph data, offering high availability, stability, scalability, and intuitiveness. We used the LOAD CSV statement of Cypher language to import data, enabling efficient real-time data insertion and facilitating future updates.
Potential Applications and Knowledge Verification
Knowledge graphs have broad applications in medicine. We integrated the knowledge graph with expert experience to explore knowledge discovery through human-computer collaboration. TCM’s experiential nature necessitates incorporating expert knowledge. Therefore, we evaluated the DKD TCM diagnosis and treatment knowledge graph by reverse validation based on expert diagnostic and treatment reasoning. The Connected Components algorithm retrieved multi-level knowledge correlations. TCM experts in nephrology and endocrinology identified critical DKD diagnosis and treatment links and posed questions. Cypher queries then verified if the knowledge graph results aligned with expert expectations and facilitated knowledge sorting and implicit treatment thinking discovery.
Five key questions, summarized after expert consultation, guided knowledge retrieval:
- Can the knowledge graph reflect the coexistence of multiple syndromes (deficiency-excess complex) in TCM diagnosis of DKD?
- Does it reflect drug adjustments (addition/subtraction) based on specific symptoms?
- Does it show instances of a single herb treating multiple symptoms during drug adjustment?
- Does treatment plan selection vary with different underlying comorbidities?
- Are there treatment option differences for the same syndrome diagnosis across different DKD stages?
Results
Ontology Concepts and Types
We defined nine ontology concepts using DKD TCM diagnosis and treatment guidelines, expert consensus, and medical record data: diseases, stages, syndrome groups, syndromes, medical examinations, symptoms, Chinese herbs, therapeutic methods, and formulae. Syndrome groups were derived from real-world data; the other eight concepts originated from guidelines and consensus (Table 4).
Table 4. Sources and definitions of ontology concepts.
| No. | Concept terms | Source | Meaning |
|---|---|---|---|
| 1 | Diseases | Guidelines, expert consensus, standards, schemes | Under the infection of the six pathogenic factors, the seven emotions, and other pathogenic factors, the internal and external environment of the body is out of balance, and then behavior and mental changes occur. It is manifested as certain symptoms and signs of pathological processes |
| 2 | Stages | Guidelines, expert consensus, standards, schemes | Diagnosis of disease severity and status |
| 3 | Syndrome groups | Real-world medical record data | In the disease process of syndrome, when one syndrome element occurs, several other syndrome elements may occur concurrently. These syndrome elements are combined to form syndrome groups |
| 4 | Syndromes | Guidelines, expert consensus, standards, schemes | The syndrome is the external presentation of the reaction status of the essential organ connection of the disease location, etiology, disease nature, disease trend, and the strength of the body’s resistance in a particular stage of the disease process, clinically observable symptoms are shown |
| 5 | Symptoms | Guidelines, expert consensus, standards, schemes | Symptoms are presentation of the abnormal status of the organ, which include various abnormal sensations felt by the patients themselves, and various abnormal manifestations sensed by the doctors |
| 6 | Medical examinations | Guidelines, expert consensus, standards, schemes | Medical examination refers to the physical or chemical test carried out in the laboratory to determine the content, properties, concentration, quantity, and other characteristics of the substances submitted for examination |
| 7 | Therapeutic methods | Guidelines, expert consensus, standards, schemes | The therapeutic method refers to the specific method of treating disease guided by the treatment principles |
| 8 | Formulae | Guidelines, expert consensus, standards, schemes | A formula is a Chinese medicine prescription composed of herbs according to the principles of compounding guidelines and the clinical experience of doctors |
| 9 | Chinese herbs | Guidelines, expert consensus, standards, schemes | Chinese herbs are natural products used for prevention, treatment, and healthcare under the guidance of TCM theory and clinical experience, including raw herbs and decoction pieces |
Alt Text: Table defining the nine core concepts within the TCM diagnosis chart’s ontology, including diseases, stages, syndromes, and treatments, detailing their sources and meanings within the TCM context.
Semantic Relationships Between Concepts
We defined nine semantic relations (object properties) between concepts: process, consisting of…, treat, coexist, use, contain, manifestation, property of, and correlation. Process, contain, manifestation, treat, use, and consisting of were derived from guidelines and consensus. Real medical record data analysis led to the addition of coexist, property of, and correlation relationships (Table 5).
Table 5. Sources and definitions of semantic relations.
| No. | Relation | Source | Meaning |
|---|---|---|---|
| 1 | Process | Guidelines, expert consensus, standards, schemes | Behavior, state, or function |
| 2 | Consist of | Guidelines, expert consensus, standards, schemes | It is used to describe the relationship between the whole and the individual. It is relative to macro description and expresses macro imagery based on segmentation |
| 3 | Treat | Guidelines, expert consensus, standards, schemes | Treatment is usually the process of intervening or changing a specific health condition. It is a process in which a means or measure acts on the human body |
| 4 | Coexist | Real-world medical record data | It is the process by which one event or activity causes another event or activity. This study refers to the process by which a pre-existing disease causes another disease |
| 5 | Use | Guidelines, expert consensus, standards, schemes | It refers to the service of instructing personnel, utilizing utensils, or funds to serve a purpose. In this study, it mainly refers to the process of using certain means or methods to treat disease |
| 6 | Contain | Guidelines, expert consensus, standards, schemes | It is the relationship between a set and a collection, also called the subset relationship. It means the existence of one thing in another |
| 7 | Manifestation | Guidelines, expert consensus, standards, schemes | The external form of things in development and change. It refers to all the situations where things are shown and felt by people |
| 8 | Property of | Real-world medical record data | A property that is unique to something, peculiar to that thing |
| 9 | Correlation | Real-world medical record data | It means that two things are related to each other. That is a shared relationship or causal relationship between things or signals |
Alt Text: Table defining the nine semantic relationships within the TCM diagnosis chart’s ontology, such as “Treats,” “Coexist,” and “Correlation,” explaining their sources and meanings in connecting different concepts.
To represent relationship strength and enhance understanding of DKD TCM diagnosis and treatment, we weighted prominent relationships based on two-dimensional relationship frequencies and categorized them into grades. This resulted in an ontological framework with nine concepts and 20 relationships (Figure 4).
Alt Text: Diagram illustrating the ontology layer of the TCM diagnosis chart’s knowledge graph for Diabetic Kidney Disease, showing the interconnectedness of concepts like diseases, stages, syndrome groups, and treatments.
DKD TCM Diagnosis and Treatment Knowledge Graph
Utilizing data mining results and incorporating relationship grades and weights, we performed standardized manual review of knowledge extraction results to correct errors and deficiencies. An EXCEL database was created for extracted results, reviewed by two experts for rationality and accuracy. The final DKD TCM diagnosis and treatment knowledge graph comprised 903 nodes and 1669 relationships.
This graph included nine conceptual nodes (“disease,” “stage,” “syndrome groups,” “syndromes,” “medical examination,” “symptoms,” “Chinese herbs,” and “formulas”) and 10 inter-nodal relationship types, connecting “disease-disease,” “disease-stage,” “disease-syndrome groups,” “stage-syndrome groups,” “medical examination-syndrome groups,” “syndrome groups-symptoms,” “therapeutic method-formulae,” “syndrome-therapeutic method,” “Chinese herbs-symptoms,” and “formulae-Chinese herbs” (Figure 5).
Alt Text: Diagram illustrating the concept and relationship distribution within the TCM diagnosis chart’s knowledge graph, showcasing connections between diseases, stages, syndrome groups, medical examinations, symptoms, and treatments with color-coded nodes and edges.
Human-Computer Interaction for Knowledge Mining and Verification
We utilized the DKD TCM diagnosis and treatment knowledge graph, which informs the TCM diagnosis chart, to extract implicit knowledge from case data, leveraging its multi-dimensional relationships and multi-hop query capabilities. The Connected Components algorithm and Cypher queries facilitated exploration and analysis. Expert-guided reverse validation assessed the graph’s performance.
Multi-hop Hierarchical Knowledge Discovery
The Connected Components algorithm enabled community clustering analysis, establishing multi-level relationships between stages, syndrome groups, syndromes, laboratory indicators, symptoms, and other entities. For example, DKD stage III and IV patients were often diagnosed with spleen and kidney yang deficiency syndrome, linked to mALB levels and a white tongue coating. Stage V patients were mainly diagnosed with water qi intimidating the upper syndrome, related to SCr levels and symptoms like vomiting, edema, abdominal distention, and cough (Figure 6). TCM experts validated these findings as clinically consistent.
Alt Text: Diagram illustrating examples of multi-level knowledge discovery within the TCM diagnosis chart’s knowledge graph using the Connected Components community algorithm, highlighting relationships between disease stages, syndromes, and symptoms.
“Deficiency-Excess Complex” in TCM Syndrome Diagnosis
Experts highlighted the frequent coexistence of multiple syndromes (deficiency-excess complex) in DKD diagnosis. Cypher queries revealed instances where multiple syndromes coexisted and were treated with the same therapeutic approach. For example, patients might present with both “Qi and Yin deficiency with blood stasis, liver-kidney Yin deficiency” and “phlegm-turbid obstruction, phlegm-blood stasis blocking collateral” syndrome groups, all treated with Qi-Yin benefiting and blood-activating, stasis-resolving methods (Figure 7). This aligns with the “deficiency-excess complex” concept, where disease progression involves coexisting syndromes and deficiency-excess mixtures.
Alt Text: Diagram illustrating the “deficiency-excess complex” concept within the TCM diagnosis chart, showing how multiple syndromes can coexist in DKD and be addressed with similar therapeutic methods.
However, experts cautioned against misinterpretations, emphasizing TCM’s principle of “treating different diseases with the same treatment” versus “treating different syndromes with the same treatment.” Treatment revolves around syndrome differentiation. The graph’s findings suggest that applying the same treatment method for different syndromes, while observed in the data, might not always align perfectly with nuanced clinical practice. Clinicians should interpret the TCM diagnosis chart with their expertise. In DKD, syndromes often exhibit “root deficiency and branch excess,” with varying degrees of deficiency and excess in syndromes like Qi-Yin deficiency and blood stasis. Clinical syndrome diagnosis must consider “deficiency and excess” and “primary and secondary” aspects, guiding treatment strategies.
Symptomatic Knowledge of Herbal Treatment Adjustments
TCM treatment is individualized, involving herb adjustments based on specific symptoms. Clinical adjustments are key in DKD TCM diagnosis and treatment. Experts raised the issue of medication adjustments. We queried the graph using Cypher for “skin itching” as an example:
MATCH (c:Chinese herb`)-[r]-(s:symptom).`
WHERE s. name = ‘Itch of skin’ RETURN c, r, s.
Semantic search revealed “symptomatic treatment” herbs. The TCM diagnosis chart can guide clinical herb selection based on weight prompts. For itchy skin, herbs like Kochiae Fructus and Dictamni Cortex showed stronger relationships and are more recommended clinically, although patient-specific factors remain crucial (Figure 8). Expert validation confirmed the retrieved herbs aligned with routine clinical medication.
Alt Text: Diagram illustrating knowledge discovery of Chinese herbs for symptom-based adjustments in the TCM diagnosis chart, specifically for skin itching, showing herbs and their weighted relationships to the symptom.
Multiple Treatments with One Herb
Chinese herbs often have multiple effects and roles across diseases and prescriptions. DKD patients have complex symptoms, and TCM practitioners often treat multiple symptoms with a single herb. We queried “multiple treatments with one drug” using Cypher, exemplified by “Poria”:
MATCH (c:Chinese herb`)-[r]-(s:symptom).`
WHERE c. name = ‘Poria’ RETURN c, r, s.
Knowledge graph retrieval showed that Poria treats various symptoms (edema, palpitation, insomnia, etc.). The TCM diagnosis chart helps identify superior herbs for specific symptoms. For example, Poria is more effective for edema and foamy urine than dry mouth (Figure 9). This facilitates rapid identification of effective treatment plans, optimizing clinical decisions. Expert verification confirmed clinical consistency.
Alt Text: Diagram illustrating knowledge discovery of multiple treatments from a single herb within the TCM diagnosis chart, using Poria as an example and showing its varied applications for different symptoms.
Comorbidities Affect Therapeutic Method Choice
Clinical diagnosis and treatment involve selecting therapeutic methods based on patient symptoms. Knowledge graph analysis revealed that comorbidity history influences treatment choices alongside symptoms and syndromes. We queried using Cypher:
MATCH(d:Disease)-[r:Coexist-strong`]->(d1:Disease), (d:Disease)-[r1:`Property of`]->(s:`Syndrome groups`)-[r2:Contains]->(s1:Syndrome)`
WHERE d. name = 'Diabetic kidney disease’ and s. name = 'Syndrome groups of dampness-heat'.
RETURN d,d1,s,s1,t,r,r2,r3.
Results indicated that damp-heat syndrome patients were treated with spleen-tonifying and qi-replenishing methods, potentially due to comorbidities like retinopathy, hypertension, and neuropathy (Figure 10). Experts validated this as improving diagnostic and treatment recommendation accuracy. Comorbidities are critical but often overlooked in DKD clinical practice. The TCM diagnosis chart, informed by the knowledge graph, considers comorbidity influence, enhancing TCM treatment efficacy for DKD.
Alt Text: Diagram illustrating how comorbidities influence therapeutic method selection within the TCM diagnosis chart, showing the impact of conditions like retinopathy and hypertension on treatment approaches for Diabetic Kidney Disease.
Stage-Dependent Treatment Plan Variations for Same Syndrome
TCM diagnosis and treatment for DKD emphasize stage-based treatment. Understanding stage and syndrome differentiation is crucial. We analyzed the knowledge graph, combined with expert inquiries, focusing on DKD stages III and IV. Cypher query:
MATCH (d:Disease)-[r:Process]->(s:Stage)
(s:Stage)-[r1]->(s1:Syndrome groups`)-[r2:Contains]->(s2:Syndrome), (t:`Therapeutic method`)-[r3:Treats]->(s2:Syndrome), (t:`Therapeutic method`)-[r4]->(f:Formula)`
WHERE s1. name = ‘Syndrome groups of Yang deficiency in spleen and kidney’ and s. name = ‘Phase III’ or s. name = ‘Phase IV’.
RETURN d,s,s1,s2,t,f,r,r1,r2,r3,r4.
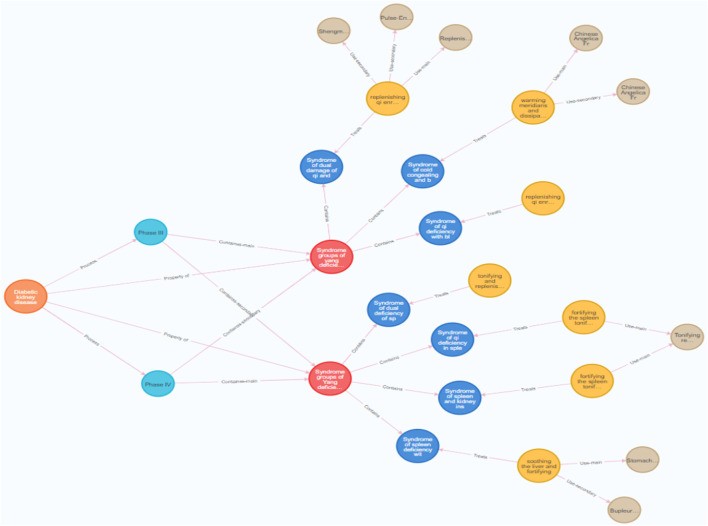
Results showed that stages influence formula choices. Spleen and kidney yang deficiency syndrome occurs in stages III and IV, most commonly in IV. Formula selection varies: Jianpi Yiqi Tiaotang Decoction or Shenqi Dihuang Decoction for spleen and kidney deficiency syndrome; Linggui Zhugan Decoction for spleen and kidney yang deficiency syndrome. Treatment option variations exist for the same syndrome group across different stages (Figure 11). The TCM diagnosis chart highlights that stages impact basic formula selection for DKD.
Alt Text: Diagram illustrating the influence of different stages and syndromes of Diabetic Kidney Disease on TCM treatment choices within the TCM diagnosis chart, showing stage-specific variations in therapeutic methods and formulae.
Discussion
Clinical decision-making is crucial in diagnosis and treatment, impacting patient outcomes. Optimal treatment plan selection is vital. TCM’s individualized syndrome differentiation makes diagnosis and treatment complex. TCM practitioner experience is invaluable but hard to access directly. Guidelines alone are insufficient for all clinical scenarios. Knowledge graphs, using algorithms to structure knowledge and relationships, effectively manage TCM data and practitioner experience. The TCM diagnosis chart is a practical application of this approach.
Knowledge graphs are increasingly used in medicine, but less so in TCM. TCM research often focuses on algorithms and model development, providing technical support for knowledge discovery but lacking clinical application guidance. Existing TCM knowledge graph research often centers on ancient literature, with limited exploration of implicit knowledge in real-world data. This gap limits clinical guidance. Furthermore, many studies focus on general knowledge graphs, lacking disease-specific graphs. Our study addresses these limitations by creating a DKD-specific knowledge graph, informing the TCM diagnosis chart, integrating guidelines, real-world data, and data mining, incorporating disease characteristics and clinical practice. This graph facilitates a holistic understanding of DKD, aiding junior doctors, enhancing diagnostic skills, and providing a methodological reference for disease-specific TCM knowledge discovery.
Limitations include single-center data, limiting data types, quantity, and representativeness of tacit knowledge. Relationships in the DKD TCM diagnosis and treatment knowledge graph also have limitations due to data constraints. Future research should incorporate multi-center data to optimize entities and relationships, uncovering more tacit knowledge to further refine the TCM diagnosis chart.
Conclusion
This study constructed a DKD TCM diagnosis and treatment knowledge graph, informing a practical TCM diagnosis chart, by combining guidelines and real-world data. Data mining-derived association weights enriched relationship types. The knowledge graph systematically organizes and visualizes fragmented DKD diagnosis and treatment knowledge. Semantic retrieval facilitated tacit knowledge discovery and sharing, enhancing DKD TCM diagnosis and treatment knowledge for junior doctors. This work supports TCM clinical guideline development for DKD and provides a foundation for an intelligent DKD diagnosis and treatment recommendation system, ultimately improving patient care.
Funding Statement
This study was supported by the China Academy of Chinese Medical Sciences Innovation Fund (No. CI 2021A00509).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by The Ethics Committee of Institute of Basic Research in Clinical Medicine, China Academy of Chinese Medical Sciences. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
TW and GP designed this study; XZ and YW processed the data; TW and YW constructed the graph; XZ, YW, and PL analyzed the knowledge obtained from the graph; GP and MQ reviewed the data and provided guidance; XZ, YW, and PL wrote the manuscript. JX and YS reviewed the article. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
[References list from original article – to be included and formatted as per requirements if needed]
Associated Data
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.