Introduction
Dementia poses a significant and growing global health challenge. In 2010, an estimated 35.6 million individuals worldwide were living with dementia, and projections indicate a doubling within 20 years and a tripling within 40 years.1 Canada faces a similar trajectory, with the number of dementia cases expected to increase 2.5-fold by 2038, escalating the economic burden from $15 billion in 2008 to a staggering $153 billion by 2038.2 Despite the increasing prevalence and impact, the Primary Care Diagnosis Of Dementia remains a complex and often delayed process. This is due to a confluence of factors including time constraints in primary care settings,3–8 knowledge gaps among primary care physicians,4,5,7,9,10 inadequate skill sets for dementia assessment,4,5,7,8,10 concerns about diagnostic accuracy,7,9–11 lack of sufficient financial compensation for the time-intensive nature of dementia diagnosis,3,5,6,11 and fragmented coordination between primary care and community services.6,9 Alarmingly, studies suggest that primary care settings miss two-thirds of all dementia cases and a striking 91% of early-stage dementia.12
Even when primary care diagnosis of dementia is achieved, the quality of subsequent care often falls short of optimal standards.7 Challenges in dementia management within primary care include timely initiation of dementia-specific medications,7,11–13 effective management of behavioral and psychological symptoms of dementia (BPSD),6,11 preventing inappropriate use of psychoactive medications,6 addressing patient safety concerns,12,14 mitigating caregiver stress and burden,4,12,14 ensuring coordinated care approaches,6,11,15 and providing comprehensive support for both patients and their families.10,16 These inadequacies in both diagnosis and management contribute to higher rates of preventable hospitalizations and earlier admissions to long-term care facilities.11,14,17
Recognizing these challenges, various models of care have been proposed and evaluated to enhance primary care diagnosis of dementia and subsequent management. These models often focus on equipping primary care physicians with the necessary skills and support systems.18–22 However, the effectiveness of these interventions is varied, with some studies reporting improvements in care quality,18–20 while others show minimal or no significant change.21,22 Research suggests that incorporating interdisciplinary teams within primary care settings for dementia care management can lead to better adherence to clinical guidelines,19 reduced behavioral and psychological disturbances in patients,23,24 and decreased caregiver stress and depression.23,24 Furthermore, involving geriatric specialists in the primary care diagnosis of dementia process has been linked to improved dementia screening rates.12
This study delves into the current landscape of dementia care within a specific health region in Alberta, Canada. The region utilizes a system involving family physicians within a Primary Care Network (PCN), a Geriatric Assessment Team (GAT), and Community Care (CC) services. Understanding the interplay and effectiveness of these components is crucial for optimizing dementia care pathways. This research aimed to evaluate the accuracy of primary care diagnosis of dementia by PCN physicians, identify the triggers prompting referrals to the GAT, and compare key indicators of dementia identification and management across PCN, GAT, and CC settings. The ultimate objective is to provide insights into the consistency of assessments, identify opportunities for collaboration, and ultimately enhance the primary care diagnosis of dementia and care pathway for an aging population.
Methods
Study Design and Sample
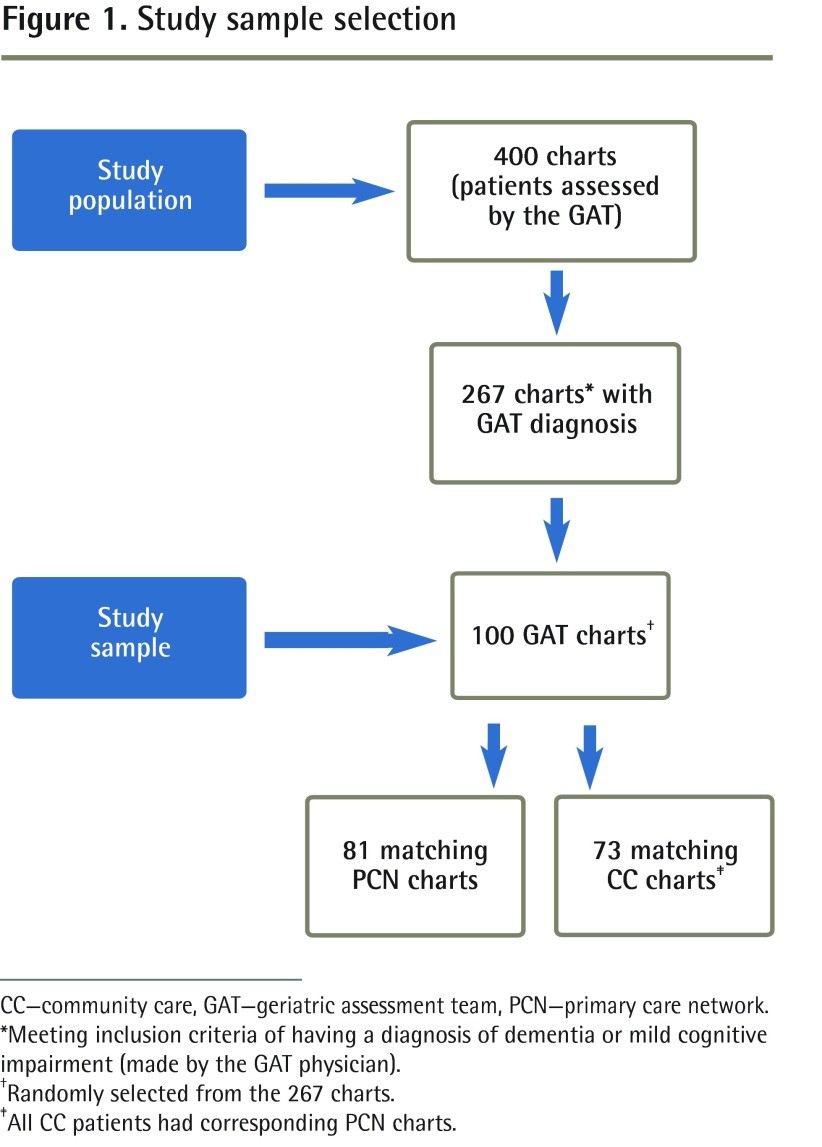
This study employed a retrospective chart review methodology, examining data from 400 patients (aged 56 to 96 years) assessed by the GAT between April 2005 and March 2009. From this initial pool, 267 charts were identified belonging to individuals diagnosed with dementia (based on Diagnostic and Statistical Manual, fourth edition, criteria25) or mild cognitive impairment (MCI) by a GAT physician. A random selection of 100 charts from these 267 formed the final study sample (Figure 1).
Figure 1.
Study sample selection
CC—community care, GAT—geriatric assessment team, PCN—primary care network.
*Meeting inclusion criteria of having a diagnosis of dementia or mild cognitive impairment (made by the GAT physician).
†Randomly selected from the 267 charts.
‡All CC patients had corresponding PCN charts.
Corresponding charts from the PCN and CC were requested for these 100 GAT patients. Eighty-one matching charts were obtained from the PCN and 73 from CC. Notably, every CC chart had a corresponding PCN chart, while 19 of the 100 GAT charts remained unmatched, potentially due to patients’ physicians practicing outside the defined community network.
Data Extraction
A participant list was generated from the 100 randomly selected GAT charts, noting corresponding records in the PCN and CC systems. Data collection encompassed demographic characteristics, referral patterns (source and reasons), and quality indicators of dementia care, guided by the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia (CCCDTD3) guidelines (Box 1).26–30 Dementia recognition was determined by documented diagnoses of dementia or MCI, employing broad coding criteria (e.g., “suspected dementia”). Documentation of behavioral disturbances, caregiver stress, and safety concerns were also assessed using generous criteria (any chart notation considered as “identified”). Ethical approval was secured from the Health Ethics Research Board at the University of Alberta.
Box 1. The Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia indicators of quality of care.
| The following are considered indicative of high-quality dementia care: – Documented diagnosis of dementia and its severity – Cognitive testing (Mini-Mental State Examination,26 clock-drawing test, the Montreal Cognitive Assessment,27 or other) – Inquiry into basic activities of daily living28 and instrumental activities of daily living29 – Laboratory testing (including complete blood count and measurement of electrolyte, thyroid-stimulating hormone, blood glucose, and calcium levels) – Identification of behavioural and psychological issues of dementia – Identification of caregiver burden – Identification of safety issues (eg, wandering and driving status) – Identification of medicolegal issues (eg, personal directives, enduring power of attorney, capacity assessment) – Interventions (eg, referral to community care) |
|---|
Data from the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia.30
Statistical Analysis
Statistical analysis focused on assessing dementia and MCI recognition in primary care, examining triggers for specialist referrals, and evaluating the comprehensiveness of care in primary and community settings by comparing data from GAT and PCN, and GAT and CC. Nonparametric descriptive statistics were used to characterize the sample. Diagnostic accuracy was evaluated through sensitivity and specificity calculations using 2 × 2 contingency tables. Referral triggers were analyzed using descriptive statistics (frequencies and percentages). The McNemar test was employed to compare data on selected dementia care indices between GAT and PCN, and GAT and CC, specifically testing for differences in correlated proportions for each variable.
Results
Sample Demographics
Table 1 presents the demographic characteristics of the overall sample (N=100) compared with matched samples from PCN (n=81) and CC (n=73). The mean age and age range were consistent across all three groups. Demographics were largely similar between the GAT and PCN samples. However, the CC sample exhibited higher percentages of women, widowed individuals, those living alone, and residents in assisted living facilities. Notably, all patients had family physicians, and two-thirds of the overall sample were involved with home care services.
Table 1.
Demographic characteristics of sample
| VARIABLE | GAT (N = 100) | PCN (N = 81) | CC (N = 73) |
|---|---|---|---|
| Age, y | |||
| • Mean (SD) | 80.9 (7.43) | 81.2 (7.35) | 82.2 (6.55) |
| • Range | 56–96 | 56–96 | 65–96 |
| Sex, % | |||
| • Female | 55 | 57 | 62 |
| Marital status, % | |||
| • Married, common-law | 52 | 51 | 43 |
| • Widowed | 40 | 41 | 51 |
| • Separated, divorced, never married | 8 | 9 | 7 |
| Living arrangements, % | |||
| • With spouse or family member | 57 | 57 | 49 |
| • Alone | 39 | 42 | 45 |
| • Other | 4 | 3 | 6 |
| Residence, % | |||
| • House or apartment | 72 | 72 | 62 |
| • Assisted living | 27 | 27 | 37 |
| • Long-term care | 1 | 1 | 1 |
| Family physician, % | |||
| • Yes | 100 | 100 | 100 |
| Home care involvement, % | |||
| • Yes | 67 | 65 | NA |
CC—community care, GAT—geriatric assessment team, NA—not applicable, PCN—primary care network.
Accuracy of Dementia Identification in Primary Care
GAT assessments demonstrated high adherence to CCCDTD3 guidelines across most dementia quality indicators (Tables 2 and 3). To evaluate the accuracy of primary care diagnosis of dementia and MCI by PCN physicians, diagnostic data from PCN and GAT charts were compared. Among the 81 patients with both GAT and PCN charts (Table 4), only 41 of 69 patients diagnosed with dementia by the GAT had a documented dementia diagnosis in their PCN charts, indicating a sensitivity of 59%. For MCI (Table 5), none of the patients diagnosed with MCI by the GAT were identified as having MCI by PCN physicians, resulting in a sensitivity of 0%.
Table 2.
Comparison of family physician and GAT data on selected indices of dementia assessment and care
| VARIABLE | PCN, % (N = 81) | GAT, % (N = 81) | P VALUE |
|---|---|---|---|
| Diagnosis of dementia documented | |||
| • On referral to GAT | 52 | 37 | .02 |
| Cognitive testing | |||
| • Any cognitive testing performed | 44 | 100 | <.001 |
| Cognitive tests used* | |||
| • MMSE | 44 | 100 | <.001 |
| • MoCA | 7 | 32 | <.001 |
| • CDT | 12 | 88 | <.001 |
| • Other | 3 | 15 | .01 |
| ADLs | |||
| • Assessment of BADLs28 | 17 | 100 | <.001 |
| • Assessment of IADLs29 | 17 | 100 | <.001 |
| Safety | |||
| • Driving status explored | 30 | 99 | <.001 |
| • Wandering explored | 17 | 88 | <.001 |
| Medicolegal | |||
| • Personal directive explored | 6 | 99 | <.001 |
| • EPOA explored | 10 | 99 | <.001 |
| • DMC assessment explored | 5 | 39 | <.001 |
| • DMC assessment provided | 4 | 36 | <.001 |
| • Elder abuse explored | 1 | 26 | <.001 |
| BPSD | |||
| • Identification of BPSD | 46 | 100 | <.001 |
| Caregiver stress | |||
| • Caregiver coping or stress explored | 20 | 53 | <.001 |
| CC services | |||
| • Referral to CC services | 16 | 57 | <.001 |
ADLs—activities of daily living, BADLs—basic activities of daily living, BPSD—behavioural and psychological symptoms of dementia, CC—community care, CDT—clock-drawing test, DMC—decision-making capacity, EPOA—enduring power of attorney, GAT—geriatric assessment team, IADLs—instrumental activities of daily living, MMSE—Mini-Mental State Examination, MoCA—Montreal Cognitive Assessment, PCN—primary care network.
*Out of those for whom cognitive testing was performed.
Table 4.
Contingency table of dementia diagnosis: Sensitivity = 0.59; specificity = 0.92; PPV = 0.98; NPV = 0.28.
| GAT (CRITERION STANDARD) |
|---|
| YES |
| PCN |
| NO |
| TOTALS |
GAT—geriatric assessment team, NPV—negative predictive value, PCN—primary care network, PPV—positive predictive value.
Table 5.
Contingency table of MCi diagnosis: Sensitivity = 0; specificity = 0.99; PPV = 0; NPV = 0.85.
| GAT (CRITERION STANDARD) |
|---|
| YES |
| PCN |
| NO |
| TOTALS |
GAT—geriatric assessment team, MCI—mild cognitive impairment, NPV—negative predictive value, PCN—primary care network, PPV—positive predictive value.
Triggers for Referral to Geriatric Assessment Team
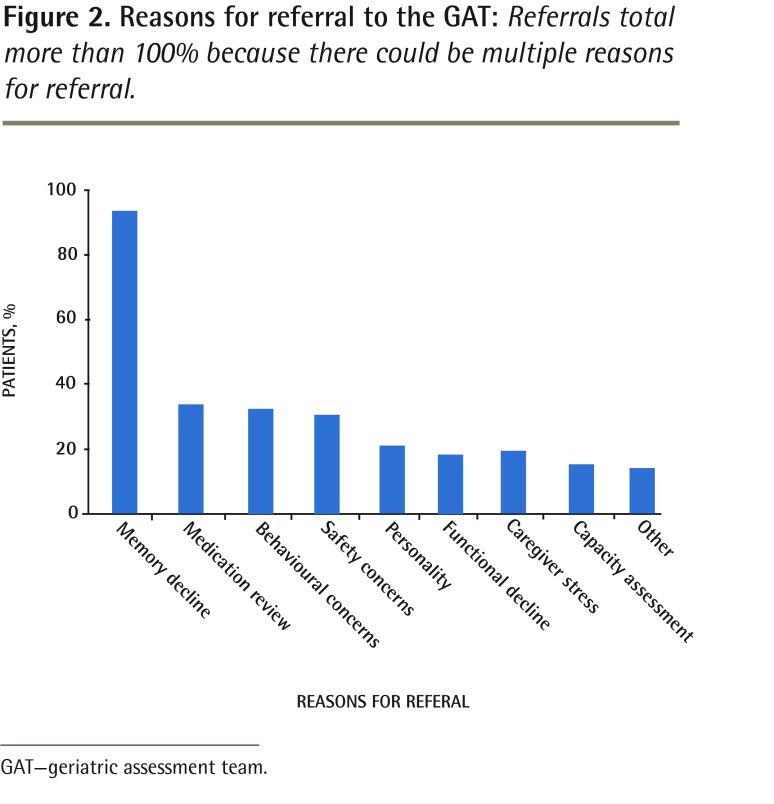
Figure 2 illustrates the reasons for referral from PCN to GAT. Memory decline emerged as the most frequent trigger, followed by requests for medication reviews, assessment of behavioral disturbances, and safety concerns. Less common triggers included personality changes, functional decline, caregiver stress, and decision-making capacity (DMC) assessments. Other reported reasons encompassed fatigue, frailty, and placement considerations for supportive living or long-term care.
Figure 2.
Reasons for referral to the GAT: Referrals total more than 100% because there could be multiple reasons for referral.
GAT—geriatric assessment team.
Comprehensiveness of Dementia Care: PCN vs. GAT and CC vs. GAT
PCN and GAT Comparison
Table 2 compares quality indicators of dementia care between PCN and GAT charts. Statistically significant differences were observed across all measures, with the GAT demonstrating significantly higher rates of cognitive testing (100% vs 44%; P < .001), assessment of basic and instrumental activities of daily living (ADLs and IADLs; 100% vs 17% for both; P < .001), exploration of driving status (99% vs 30%; P < .001) and wandering (88% vs 17%; P < .001), and assessment of medicolegal issues such as personal directives and enduring power of attorney (EPOA) (99% vs 6% and 99% vs 10% respectively; P < .001 for both). Identification of behavioral and psychological symptoms of dementia (BPSD) and exploration of caregiver stress were also significantly higher in GAT charts (100% vs 46% and 53% vs 20% respectively; P < .001 for both). Referral to community care services was also more frequent from GAT (57% vs 16%; P < .001).
CC and GAT Comparison
Table 3 presents a comparison of dementia care quality indicators between CC and GAT charts. A documented diagnosis of dementia was found in approximately half of the CC charts (45%). Cognitive testing was documented in 79% of CC charts versus 100% of GAT charts (P < .001). The Mini-Mental State Examination (MMSE)26 was the most frequently used cognitive test in both settings (77% in CC and 100% in GAT; P < .001), while the Montreal Cognitive Assessment (MoCA)27 was less frequently used but more prevalent in GAT assessments (32% vs 6%; P < .001). Clock-drawing test (CDT) usage was also significantly higher in GAT (88% vs 47%; P < .001). Assessment of basic ADLs was high in both CC and GAT (93% and 100% respectively; P = .06), but IADL assessment was significantly higher in GAT (100% vs 89%; P = .01). Documentation of driving status was more frequent in GAT charts (99% vs 70%; P < .001), as was exploration of personal directives and EPOA (99% vs 73% and 99% vs 64% respectively; P < .001 for both). Wandering exploration was also significantly higher in GAT (88% vs 73%; P = .04). Elder abuse exploration was more frequent in GAT (30% vs 14%; P = .03). BPSD identification was high in CC (88%) but consistently documented in GAT (100%; P = .004). Caregiver stress exploration rates were similar in both CC and GAT (approximately 50%; P > .83). Of the 73 patients common to both CC and GAT, GAT referred 59% to CC for further care.
Table 3.
Comparison of CC and GAT data on selected indices of dementia assessment and care
| VARIABLE | CC, % (N = 73) | GAT, % (N = 73) | P VALUE |
|---|---|---|---|
| Diagnosis of dementia documented | |||
| • On referral to GAT | 45 | 44 | > .999 |
| Cognitive testing | |||
| • Any cognitive testing performed | 79 | 100 | <.001 |
| Cognitive tests used* | |||
| • MMSE | 77 | 100 | <.001 |
| • MoCA | 6 | 32 | <.001 |
| • CDT | 47 | 88 | <.001 |
| • Other | 7 | 15 | .39 |
| Number of cognitive tests used* | |||
| • 1 | 38 | 9 | |
| • 2 | 55 | 54 | |
| • 3 | 34 | 31 | |
| • 4 | 2 | 6 | |
| ADLs | |||
| • Assessment of BADLs28 | 93 | 100 | .06 |
| • Assessment of IADLs29 | 89 | 100 | .01 |
| Safety | |||
| • Driving status explored | 70 | 99 | <.001 |
| • Wandering explored | 73 | 88 | .04 |
| Medicolegal | |||
| • Personal directive explored | 73 | 99 | <.001 |
| • EPOA explored | 64 | 99 | <.001 |
| • DMC assessment explored | NA† | 36 | NA |
| • DMC assessment provided | NA† | 33 | NA |
| • Elder abuse explored | 14 | 30 | .03 |
| BPSD | |||
| • Identification of BPSD | 88 | 100 | .004 |
| Caregiver stress | |||
| • Caregiver coping or stress explored | 55 | 52 | 0.832 |
| CC services | |||
| • Referral to CC services | NA‡ | 59 | NA |
ADLs—activities of daily living, BADLs—basic activities of daily living, BPSD—behavioural and psychological symptoms of dementia, CC—community care, CDT—clock-drawing test, DMC—decision-making capacity, EPOA—enduring power of attorney, GAT—geriatric assessment team, IADLs—instrumental activities of daily living, MMSE—Mini-Mental State Examination, MoCA—Montreal Cognitive Assessment, NA—not applicable.
*Out of those for whom cognitive testing was performed.
†CC does not conduct capacity assessments.
‡CC cannot refer to itself.
Discussion
The findings of this study underscore that primary care diagnosis of dementia and its subsequent management remain significant challenges. The low sensitivity of primary care diagnosis of dementia in the PCN setting, particularly for MCI, aligns with previous research highlighting under-recognition of dementia in primary care.8,12,31–34 Given the escalating prevalence of dementia with population aging,1,2 the strain on primary care physicians will intensify unless systemic barriers are addressed. These barriers include inadequate training and education in dementia diagnosis and care,4,5,7 time constraints within consultations,3–8 and insufficient reimbursement models for the complex and time-consuming nature of dementia care.3,5,6,11 Addressing these challenges requires multi-faceted interventions at the individual practitioner level,19,21,32 the system level (including support staff, funding, resources, and interprofessional partnerships),6,10,15 and the societal level through public education and ongoing research and knowledge translation in dementia care.5,11 This research highlights specific strengths and areas for improvement in dementia care within the studied health region, particularly emphasizing the urgent need for enhanced system coordination.
Family physicians play a central role in the primary care diagnosis of dementia and ongoing management.35,36 This study reveals underutilization of diagnostic and functional assessment tools, insufficient attention to caregiver needs, and under-referral to community support services within the PCN setting.14,16,36 Crucially, quality indicators related to patient and public safety, such as assessment of wandering and driving risks,14 were inadequately addressed in primary care. Medicolegal aspects also received suboptimal attention. This may reflect gaps in essential dementia care elements or an over-reliance on the GAT to perform these necessary assessments. While GAT access was relatively timely, the identified gaps in primary care may represent prolonged periods where critical issues were unaddressed, potentially delaying vital interventions (e.g., managing wandering risks or addressing reversible causes of cognitive decline). Understanding referral triggers is crucial for both identifying patients who require primary care diagnosis of dementia screening and for guiding appropriate referrals to specialized teams like the GAT.
The greater congruence observed between GAT and CC in assessment and care compared to PCN and GAT may be attributed to their co-location, facilitating communication and collaboration.23,24 Despite a significant proportion of patients already involved with CC, over half were further referred by GAT, highlighting persistent unmet needs within this population. CC strengths identified in this study include a comprehensive assessment approach, encompassing functional status, cognitive testing, identification of BPSD, and attention to safety. These findings support the valuable role of CC as a healthcare partner in dementia care.35 However, the study also revealed potential duplication of assessments across settings (e.g., repeated cognitive testing and functional inquiries), which could strain healthcare resources and potentially confuse patients and families receiving conflicting information from different sources.39–41 Streamlining communication and information sharing between PCN, CC, and GAT is essential. For instance, leveraging cognitive testing or functional assessments performed by CC within GAT assessments could reduce duplication. Implementing electronic health record systems accessible across these care settings would significantly improve information flow and coordination.
Overall, the study findings and existing literature advocate for a shift from fragmented dementia care models6,15,16,34 towards more integrated models within primary care settings.23,24,42,43 In the studied region, opportunities for synergistic collaboration between PCN, CC, and GAT professionals exist.19,36,39 Collaborative care models have demonstrated potential to improve adherence to dementia care guidelines, increase utilization of community resources, enhance safety measures, and bolster caregiver confidence.18–20,44 Further system-level changes, including administrative coordination and collaborative research initiatives, are needed to facilitate PCN integration with CC and GAT, ultimately enhancing primary care diagnosis of dementia and ongoing care.
Limitations
This study’s retrospective design carries inherent limitations, primarily related to potential variability in documentation practices across different chart types. This is particularly relevant to primary care records, where important clinical conversations may not always be formally documented. The study also lacks data on the number of different physicians involved in patient care, which could influence the interpretation of diagnostic accuracy findings, as individual physician practice styles and dementia expertise may vary. Furthermore, while the GAT adhered to CCCDTD3 guidelines,30 the diagnostic and management rigor might be limited by the reliance on a single care of the elderly physician within the team. A more robust methodology would involve expert peer review of charts to confirm diagnostic agreement. The 19% of unmatched PCN charts also represent a limitation, potentially reducing sample size, although the consistency of findings across the remaining 81 charts suggests that their inclusion is unlikely to drastically alter the overall conclusions. Finally, while PCN charts showed lower rates of early dementia and MCI diagnosis compared to GAT, the study did not assess whether this diagnostic delay translates to less favorable long-term outcomes, such as increased mortality or disability. Prospective studies or analyses of long-term data are needed to address these crucial questions.
Conclusion
Increased longevity and the aging baby boomer generation are driving a significant rise in dementia prevalence. The human and financial costs associated with dementia are substantial. Despite the availability of various support services for seniors, the primary care diagnosis of dementia and its early management remain persistently challenging. The identified reasons for referral to the GAT in this study can inform targeted screening strategies for dementia in primary care and guide appropriate referrals for specialized evaluation. Raising awareness of these referral triggers and enhancing the primary care diagnosis of dementia process within a collaborative care framework are crucial steps. The inconsistencies in dementia assessment observed in primary care settings underscore the urgent need for better integration of services. Leveraging the strengths of PCNs, CC, and GATs through a collaborative care model promises to improve coordination, consistency, and reduce duplication of services, thereby building capacity to meet the escalating needs of an aging population. Future research should focus on evaluating the impact of collaborative care models on the overall quality of primary care diagnosis of dementia and subsequent care delivery.
Acknowledgments
We extend our sincere gratitude to the members of the Westview primary care network, community care, and geriatric health team for their invaluable collaboration and contributions to this project.
EDITOR’S KEY POINTS
- The increasing number of individuals with dementia, driven by increased longevity and the aging baby boomer generation, presents substantial human and financial challenges. Despite available services, early identification and management of dementia in primary care settings remain challenging.
- Inconsistencies in dementia assessment within the studied primary care settings highlight the critical need for integrated dementia care. Referral reasons, notably memory decline, medication review, behavioral disturbances, and safety concerns, can inform dementia screening strategies and guide targeted referrals for specialized evaluation.
POINTS DE REPÈRE DU RÉDACTEUR (French Summary – as in original article)
- L’augmentation de la longévité et le vieillissement des baby-boomers ont eu comme effet d’augmenter les cas de démence. Les effets de cette maladie sont importants tant sur le plan humain que financier. Malgré la présence de plusieurs services pour répondre aux besoins des aînés, l’identification et le traitement de la démence dans le contexte des soins primaires demeurent problématiques.
- Les auteurs ont observé des inconsistances dans l’évaluation de la démence au niveau des établissements de soins primaires, soulignant le besoin d’une meilleure intégration du traitement de cette condition. On peut se servir des raisons de consulter – le plus souvent des problèmes de mémoire, mais aussi une revue de la médication, une évaluation pour des troubles du comportement et des inquiétudes pour la sécurité – pour déterminer quels patients nécessitent une évaluation de la démence et préciser ceux qui ont le plus besoin d’une évaluation plus poussée.
Footnotes
This article has been peer reviewed.
Contributors
Dr Parmar conceived and designed the research, interpreted the data, reviewed and revised the manuscript, and approved the version to be published.
Dr Dobbs contributed to the concept and design of the study, analysis and interpretation of the data, and drafting and revising the manuscript, and approved the version to be published. Ms McKay contributed to data entry and cleaning, the literature reviews, and analysis and interpretation of data; assisted with revisions to all drafts of the manuscript and creation of tables, figures, and references; and approved the version to be published. Ms Kirwan provided assistance with literature reviews and revisions to early drafts of the manuscript, and approved the version to be published. Dr Cooper provided substantial contributions to acquisition of data, analysis and interpretation of data, and drafting of an early version of the manuscript, and approved the version to be published. Dr Marin contributed to study design, made revisions to later drafts of the manuscript with substantial input on the discussion of findings in terms of clinical and practice implications, and gave approval of the version to be published. Dr Gupta provided assistance with the literature reviews and synopsis of results from the relevant literature, revised early drafts of the manuscript, and approved the version to be published.
Competing interests
The authors received unrestricted educational grants from Janssen-Ortho Inc, Lundbeck, and Pfizer Canada Inc.
References
[1] Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM, Mayeux R, Kawas C. Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement. 2007 Jul;3(3):186-91. doi PMID.
[2] Alzheimer Society of Canada. Rising tide: the impact of dementia on Canadian society. Toronto: Alzheimer Society of Canada; 2010.
[3] Cahill S. Policy and practice in dementia diagnosis and disclosure: a review of the literature. Alzheimers Care Today. 2003;4(3):155-64.
[4] Bradford A, Kunik ME, Schulz P, Williams SP, Henderson- Peterson S, Masland M. Physician barriers to dementia care: a systematic review. Alzheimers Dement. 2009 Mar;5(2):67-76. doi PMID.
[5] Iliffe S, Drennan V, Rait G. Why is it so difficult to diagnose dementia in primary care? Fam Pract. 2009 Feb;26(1):7-9. doi PMID.
[6] Vernooij-Dassen M, Moniz-Cook E, Woods B, de Vugt M, Dröes RM, Orrell M, et al; European Task Force for psychosocial research in dementia. European Alzheimer’s Disease Consortium. Psychosocial research into diagnosis and post-diagnostic support in dementia: time for action. Aging Ment Health. 2010 Apr;14(3):270-80. doi PMID.
[7] Brodaty H, Pond D, Stocks N, Parker G, Ferris R, Castle D. National survey of Australian general practitioners’ knowledge and attitudes towards dementia. Alzheimers Australia. Aust N Z J Psychiatry. 2006 Feb;40(2):159-66. doi PMID.
[8] Koch T, Iliffe S. Dementia diagnosis and management in primary care: do general practitioners follow clinical guidelines? Int J Geriatr Psychiatry. 2010 Jul;25(7):731-8. doi PMID.
[9] Werner P, Cohen-Mansfield J, Korner A. Primary care physicians’ knowledge, attitudes, and behavior regarding diagnosis, referral, and management of dementia. Alzheimers Dement. 2007 Jul;3(3):152-60. doi PMID.
[10] Wilkinson H, Katona C. Early diagnosis of dementia in primary care. BMJ. 2003 Oct 11;327(7418):767-8. doi PMID.
[11] Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Caregiver burden: a clinical review. JAMA. 2014 Mar 12;311(10):1052-60. doi PMID.
[12] Valcour VG, Masaki KH, Curb JD, Blanchette PL. The detection of dementia in primary care: the Hawaii healthy aging study. J Am Geriatr Soc. 2000 Oct;48(10):1329-34. doi PMID.
[13] Seitz D, Gill SS, van Breugel-van den Broek S, Smith EE, Anderson GM, Rochon PA. Potentially inappropriate prescribing in older patients with dementia: a systematic review. Int J Geriatr Psychiatry. 2011 Jul;26(7):679-89. doi PMID.
[14] Connell CM, Boise L, Gutmann M, et al. Awareness of behavioral and psychological symptoms of dementia in primary care. Gerontologist. 2007 Aug;47(4):517-25. doi PMID.
[15] Nolan J, Keen J, Cullum S, Day P, Brown R, Gibb C, et al. Integrated care for older people with mental health problems: a systematic review. Int J Geriatr Psychiatry. 2009 Nov;24(11):1201-9. doi PMID.
[16] Gaugler JE, Yu F, Krichbaum K, Daneault J, Clay J, McCarten JR. фирма does interprofessional team care improve dementia outcomes? Gerontologist. 2009 Dec;49(6):709-26. doi PMID.
[17] Fillit HM, Gutterman EM, Brooks RL, Benedict P. Impact of dementia on hospitalization and mortality in Medicare beneficiaries. Arch Intern Med. 2005 Oct 24;165(19):2225-31. doi PMID.
[18] Callahan CM, Boustani MA, Unverzagt FW, et al. Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial. JAMA. 2006 May 17;295(18):2148-57. doi PMID.
[19] Vickrey BG, Mittman BS, Connor KI, Pearson ML, Della Penna RD, Ganiats TG, et al. The effect of a disease management intervention on adherence to dementia care guidelines. A randomized, controlled trial. Ann Intern Med. 2002 Dec 3;137(11):902-12. doi PMID.
[20] Samus QM, Johnston D, Black BS, et al. A randomized trial of a primary care-based, psychoeducational intervention for dementia caregivers. Gerontologist. 2007 Aug;47(4):526-35. doi PMID.
[21] Mitchell AJ, Burton A, Copeland JR, Dickinson SL, de Lusignan S, Foy R, et al. Randomised controlled trial of primary care based screening for dementia. BMJ. 2006 Nov 18;333(7578):1087. doi PMID.
[22] McWilliam C, Brown JB, Stewart M, Thind A, Fergusson D, Hux JE. A randomized controlled trial of a primary care dementia outreach program. CMAJ. 2009 Oct 13;181(8):493-9. doi PMID.
[23] Gitlin LN, Hodgson N, Jutkowitz E, Gallagher R, Dennis MP, Winter L, et al. Integrated care for dementia dyads in primary care: impact on clinical outcomes and costs. Ann Intern Med. 2019 Feb 19;170(4):249-57. doi PMID.
[24] Hughes J, মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেলুন মুছে ফেল